1. Foreword
Quite some time has elapsed since Fleur Loveridge asked me if I could write a fuller account of the caving "career" of Włodek Szymanowski, a Polish caver who had long ties to OUCC and who had died in a diving accident in April 2005. I had already written an obituary about him that was full of relevant, and sometimes amusing, anecdotes and wanted to avoid simply writing an "obit+". Additionally, I wasn't sure that there were enough further anecdotes to fill a new article in a similar vein. Since I have only a limited picture of Włodek's caving career, I asked around for further information and, if possible, for further amusing anecdotes. People seemed to be enthusiastic but memories aren't what they used to be and the promised information and/or photos tended not to be to hand but might be located in the basement/attic/parents' place/wherever. Despite gentle reminders from time to time, little of substance subsequently appeared. That said, an old friend of Włodek did give me one amusing anecdote: While caving with a group of Poles in Spain, Włodek had been on one particularly long underground trip. Knowing how ravenous the underground team would be on their return, the surface team prepared a salad for them and then went to bed. In the morning the surface team got up to find that the Włodek & co. had returned in the night but the salad remained uneaten. Somewhat bemused, they investigated further and found that the waste container, full of pepper cores, vegetable peelings and generally disgusting pieces of food detritus, had been emptied overnight…
So, I've finally had to admit defeat on Plan A. This article is Plan B, but I hope people nevertheless still find it interesting and relevant. While Włodek had been an outstanding caver of his generation, it was only in the last 4 years of his life that he took up cave diving. I also hope that the article and its necessary technical content might be of wider interest than one based solely on the life of a guy that many newer OUCC members never met.
I have tried to make this article as accessible as possible to all readers and it is therefore not written in the style of an academic paper. It covers a technical subject, and to understand what went wrong the reader needs a basic knowledge of some dive theory and how a rebreather system works. There is therefore, of necessity, a rather long introduction so that the non-diver is able to understand the fundamentals of these two subject areas. This has increased the length of the article considerably but I see little alternative. Complicated formulae have also been avoided and worked examples used to illustrate concepts that might be new to the reader.
I am not a diver and in order to write this article I have had to "push the envelope" of my diving knowledge and might have made some fundamental errors. The conclusions I have reached have had to be based upon sometimes ambiguous and often incomplete information I have managed to unearth. As research for this article has progressed, I have, on several occasions, changed my view about what I believe probably occurred, and would not for one minute claim to have the last word on the matter. Although the root cause of the accident has been identified with a high degree of certainty, it has proved impossible to say with the same degree of certainty how it led to Włodek's death. The following section, in which I try to recreate the accident itself, should therefore be taken as my best guess as to what happened, given the available evidence.
Finally, I'd like to thank Tony Seddon, Chris Densham, Sebastian Dobrowolski, Mirek Kopertowski and Paweł Mordkowicz for their help in providing useful information and guidance during the writing of this article. A special thanks must also be given to Ian Robertson of Analox Ltd for the unfailing help he gave me in understanding the ins and outs of breathing gas physics.
Martin Hicks
2. Depth in the Morning
The picturesque French town of Bourg Saint Andéol probably seemed a good place to be on that April morning in 2005 as Włodek Szymanowski kitted up. With its pretty, limestone-built houses and narrow, cobbled streets, it would grace any postcard and no doubt sees many tourists during the warmer months of the year. Włodek's business in the town that April morning was also tourism, of a sort, namely cave tourism – specifically cave-diving tourism. For Bourg Saint Andéol is the home of some magnificent flooded cave systems and Włodek was about to explore one of them.
The cave he had chosen for that day's dive was the Goul du Pont, a completely flooded system that is entered via a 3-4 metre diameter walled-off pool situated under an arched railway viaduct. The dive promised to be a good one. Not only was the cave reputed to contain splendid, spacious passages and crystal clear water but it was also very deep, having already been pushed to -178m by French explorers. While Włodek was not equipped to reach such a depth, this dive was nevertheless an opportunity to see many of the splendid submerged passages and, perhaps, finally to better his personal depth record of -102.7m that he'd set some two years previously.
Deep dives, such as the one Włodek was preparing to undertake, require a high level of expertise and specialised equipment. By now Włodek had acquired both, having been actively cave diving for four years, and had become one of the leading experts within Poland in what is sometimes referred to as "technical diving". For this dive he would use his much trusted "Buddy Inspiration" rebreather equipment and would breathe a specialised gas mixture – known in the jargon as a trimix – formulated for deep diving.
That morning there had been some minor damp-related problems with his rebreather as a result of residual water from a short dive he'd done the previous evening, but nothing to cause him undue worry or force him to abort the dive. The previous evening's dive also proved that the equipment was functioning correctly, so it was all systems go for the Goul du Pont.
The Buddy Inspiration is a computer-controlled technical marvel of sub-aqua engineering that is used as a replacement for the traditional "Jacques Cousteau" type of scuba equipment. In the right circumstances, a rebreather can allow a diver to stay underwater longer and generally extend a diver's underwater capabilities. As with so many things, all this comes at a price: higher initial cost and higher technical complexity before and during use. It's probably also fair to say that the scope for potential problems is also extended. But all of this techie complexity was just what Włodek liked. His fascination with gadgets was legendary, as was his love of risk taking.
He stepped into the entrance pool and attached to his harness two 10-litre cylinders, each weighing around15kg, that had been pre-placed in the water. The cylinders, each equipped with a breathing regulator, were a critical safety backup in the case of rebreather failure underwater. In an emergency, either could be used independently of the rebreather, with one containing a trimix designed for emergency use in the deeper parts of the cave and the other containing a gas mixture for the shallower depths. After performing the long-winded but necessary pre-dive checks on his rebreather, Włodek's head dipped below the water and he began his dive.
The equipment he was wearing was very bulky and not ideally suited to caves where space is generally restricted. The rebreather was back-mounted and covered in a hard, yellow, turtle-like shell, which placed a limit on the height of passage through which he could easily move. Plus, the side-mounted safety cylinders added a further challenge to negotiating his way through any restricted spaces. While such a set-up offers no such problems when used in open water, its use could be problematic in smaller caves. Fortunately, apart from a brief shingle-filled constriction near the entrance, at a depth of -12m, the Goul du Pont is generally spacious and ideally suited to the bulky equipment he was wearing.
Open-water diving on conventional equipment can be complicated enough for many people. For the rebreather diver, the list of tasks that must be performed as the diver descends is significantly extended. As he descended, Włodek had many things to keep himself busy, in addition to enjoying the spectacle of the cave passage around him. One of the most important of these tasks was regular and frequent monitoring of the oxygen level of the gas he was breathing. In theory, the rebreather's automated control system should be able to regulate the oxygen level with a high degree of accuracy, but computer control still has its limitations and can malfunction, so a close eye needs to be kept on the readings at all times. For each metre of depth gained (or lost on the ascent), the diver must add (or remove) an appropriate amount of gas from the rebreather in order to equalise the breathing gas pressure with the outside water pressure. Without this simple task, which was a manual operation on Włodek's equipment, breathing would quickly become impossible. Similarly, pressure adjustment must be made to the diver's dry suit to keep it at its optimum inflation level and avoid it pinching the diver's skin as depth increases (or ballooning as pressure decreases on the ascent). The same applies to the diver's buoyancy control device which, as the name suggests, is used to regulate the diver's buoyancy. On top of this, there are other tasks such as the regular monitoring of gas pressure in the cylinders, dealing with the dive computer, monitoring depth, carefully controlling the rate of descent (or ascent)and time underwater. All this, and more, while still remembering to breathe and find your way through the cave.
After the shingle constriction, Włodek reached a relatively horizontal piece of passage that quickly widens out. The water was, as expected, exceptionally clear that day and his helmet-mounted lights would have pierced the darkness with ease, allowing him to see far ahead into the inky distance. Then, at a depth of -18m, and just 75 metres from the entrance, the cave passage changes direction abruptly and plunges headlong into the depths. This is where the real challenge of the cave begins.
For those unfamiliar with diving, following the passage down was not simply a matter of Włodek rotating his body into a vertical position, with his head pointing down, and going for it. A diver, particularly when using the Buddy Inspiration rebreather, needs to maintain a relatively horizontal position in the water. Descent and ascent are normally controlled by regulating the buoyancy of the diver: reduce the buoyancy to descend and increase the buoyancy to ascend. Thus, to go down the diver releases some air from a buoyancy control device (BCD) attached to the diver. Similarly, adding air to the BCD will increase its buoyancy. The one complication is that as the diver descends the water pressure progressively compresses the remaining air in the BCD causing an equally progressive loss in its buoyancy and, if nothing further is done, will lead to an ever faster rate of descent until the diver hits the bottom. So, to maintain a controlled rate of descent, the diver must regularly add new air to the BCD as depth increases. To halt the descent and gain neutral buoyancy, the diver needs to add a larger squirt of air to the BCD – but not too much or he'll start to rise. To begin the descent Włodek released a small amount of air from his BCD and began to drift gently downwards.
The next 60 metres of depth involve a series of vertical steps in classic phreatic-shaped passage. The route is lined and, with the clear conditions that day, route finding would have been no problem. At some point during this portion of the descent, Włodek probably began to experience some unexpected problems. First was that the effects of nitrogen narcosis that day probably seemed to be greater than he was expecting and, as he descended beyond -50m, became progressively worse. The actual effects of nitrogen narcosis on a diver's physical and mental capabilities can vary greatly from day to day, even for the same person, so, although narcosis would almost certainly have affected him, it is impossible to say how serious it would have been on this occasion. What can be said with more certainty is that Włodek was not one to let minor setbacks get in the way of an important goal, so was unlikely to have been put off by what he might have perceived to be "just a bad day". Secondly, we can say with a greater degree of certainty that he would have had to work harder to breathe than was normally the case, and that the deeper he went, the worse this problem would become. Again, he might simply have pushed the problem to one side and convinced himself that he was just having a bad day, or perhaps his perception of the problem was already being dulled by the effects of nitrogen narcosis.
At a depth of -79m, the series of vertical steps ends and a horizontal gallery is entered. Although by this depth there was a very high probability that he was affected by nitrogen narcosis and that breathing was unusually difficult, he nevertheless pushed on along the gallery to the head of the magnificent 30m pitch.
It is always difficult to be sure of the motivation behind a person's actions but the decision to press on would have been made in the knowledge that the pitch is a very fine example of its kind and that its final depth of around -110m gave him a chance to beat his personal depth record. And, as we know, Włodek was a strongly self-motivated individual who didn't like to allow minor inconveniences to sidetrack him from his goals. He positively relished adversity and challenge, since they made the final victory even sweeter. Very possibly narcosis was also adversely affecting his ability to analyse his situation and take critical decisions. This was the crux of the dive and, instead of turning back, as he clearly should have done, he continued with the dive, in spite of the difficulties he would have been experiencing at this point.
To proceed along the horizontal gallery, he would have slightly inflated his BCD so as to give himself neutral buoyancy. To descend the pitch, he now needed to vent off a small amount of air from the BCD in order to achieve a slight negative buoyancy.
As he slowly descended the pitch, the symptoms he had experienced earlier are almost certain to have worsened with each metre of depth added. Progressively increasing narcosis would have adversely affected both his ability to operate the complex diving equipment he was wearing and his perception of the situation in which he found himself. Even if the automatic systems of the rebreather were functioning correctly, Włodek still needed, for example, to regulate the gas pressure within his rebreather and control the rate of descent via his BCD. In addition to the ever-increasing narcosis, the gas he was breathing also became denser and, as a consequence, it would have become increasingly difficult to breathe. This was fundamental physics at work. The simple act of breathing was becoming ever more tiring as he forced the increasingly dense breathing gas into his lungs and then back through the rebreather system. Instead of slowly drifting down the pitch in a relaxed and leisurely manner he found he was having to work progressively harder simply to breathe.
While the problem of increasing gas density is, to some degree, inherent in all deep diving, we can be fairly sure that Włodek's experience would have been at the extreme end of the scale. Normally, the act of working hard can require an increase in the rate of breathing so as to take on fresh oxygen and eliminate carbon dioxide. When it is the act of breathing itself that causes a further increase in the rate of breathing, the situation can quickly get out of hand. The problem can be further exacerbated by the reduction in efficiency of the lungs known to occur at depth, so that insufficient oxygen may be taken in through the lungs and insufficient carbon dioxide expelled from the bloodstream. To make matters worse, there is some doubt as to whether Włodek's rebreather was able to deal efficiently with exhaled carbon dioxide when at great depth, and it is possible that he was re-breathing some exhaled carbon dioxide. All things said, his situation was becoming increasingly precarious with each metre of depth gained.
What happened next can only be a matter of speculation, based upon the very sparse evidence available. A likely scenario is that, in his increasingly narcotic and befuddled state, at a depth of somewhere around 90-100m narcosis simply overwhelmed his ability to regulate his buoyancy and, very possibly, control the gas pressure within his rebreather. As he drifted downwards out of control, he came to rest on a ledge at a depth of -105m.
By now he would have been, at best, in a partially-conscious state but perhaps the impact of hitting the ledge or the inability to breathe briefly jolted him into action. He still had one ace up his sleeve. The rebreather had a modification that allowed him to switch from the main rebreather circuit and breathe directly from one of its small onboard cylinders. The logic was that even if the rebreather had somehow malfunctioned, the onboard cylinder should not be affected by the malfunction. Theoretically, the small cylinder contained enough gas to last him only 60-90 seconds but that should normally be sufficient time for him to get off the rebreather and onto the external emergency cylinder.
He turned the switch and would have found that he could once again breathe. Unfortunately, he was by now capable of doing very little else. He lay there, physically and mentally unable to make the relatively simple, but absolutely crucial, move over to his attached emergency cylinder, which remained untouched. Within less than a minute of the switch over to the onboard cylinder, the mouthpiece left his mouth and he drowned. He was 46 years old.
3. Beginnings
In late December 2000, Włodek Szymanowski made one of his his regular journeys to the Polish Tatra mountains to do a spot of winter caving. By the time he returned home, a week or so later, he was a dissatisfied man. He was by then 42 years old and had witnessed a younger generation of cavers going boldly where he had never gone before: into sumps. Of course, he had free-dived sumps in his time and had, for example, done the Swildon's Long Round Trip without a wetsuit, but these guys were doing the real deal. For Włodek, the darkness – of the open-air variety – had long ago beckoned but this time it was the vodka-clear sumps in the Western Tatras that had finally fired-up his motivation. He had long considered getting into cave diving but this time resolved to remedy the situation, and by then had the financial means to do so.

Fast-forward to March 2001 and Włodek is sitting next to a swimming pool in Hurghada, Egypt, a resort on the Red Sea coast famous for its diving. Scattered around the poolside is a group of his colleagues from the Warsaw office of Siemens Financial Ltd. Incredibly, Włodek had managed to persuade his employer that it would be A Good Thing if he and his team were to fly off to do a bit of *cough* "team integration" – and where better than at a warm-water tourist resort that happens to be a mecca for open-water diving. Once there, he enrolled on a diving course and took the first steps towards his goal of becoming a cave diver. He returned home proudly holding a PADI "Open Water Diver" certificate, dated 13 March 2001.
In spite of an earlier assurance to his wife that he would not take up cave diving, by June 2001 Włodek had consulted with one of Poland's leading cave divers at the time, Wiktor Bolek, had bought enough kit to get started and had enrolled himself on a cave-diving course. In August 2001, Wiktor Bolek led a Polish cave diving expedition to a large resurgence, Izbucul Tauz, in the Bihor region of Romania, a place he [Wiktor] had first visited in February, and, as a rookie diver, Włodek went along. But being a rookie didn't stop him diving to a depth of -50m. It was on this expedition that the Polish cave divers first tested a rebreather unit, the Buddy Inspiration.
With the zeal of the convert, Włodek went about getting as much training under his weight-belt as possible. These are just the official courses I could easily find, although he almost certainly took more:
|
Date |
Course |
|
6 October 2001 |
PADI Advanced Open Water Diver |
|
13 October 2001 |
TDI Qualified in use of 22% to 40% nitrox to 40m |
|
1 April 2002 |
TDI Qualified in all standard and custom nitrox to 45m |
|
3 April 2002 |
TDI Qualified in semi-closed rebreather technology |
|
10 April 2002 |
TDI Qualified in no-decompression dives with Buddy Inspiration rebreather to 40m using normoxic diluent |
|
27 May 2002 |
Extended range diving and decompression techniques to 55m using compressed air and nitrox/oxygen |
The astute reader might notice the reference to the Buddy Inspiration rebreather in the 10 April 2002 course, the same model that had been tested by the Poles in August 2001. That is because Włodek had received a generous year-end bonus from his employer at the end of 2001 and had blown a large portion of it on new diving kit, including the aforementioned rebreather. It appears that he was uncharacteristically cautious about using the new gadget and got some real training in its use before trying it in earnest. Since this is an article that looks at how Włodek died, it will focus on the rebreather technology he was using at the time of the accident, with particular emphasis, where applicable, on the Buddy Inspiration rebreather, manufactured in the UK by Ambient Pressure Diving Ltd.
4. Open Circuit Diving
The following will probably be a little tedious to any diver, who will probably want to skip this section (or even next two sections), but nevertheless needs to be explained for the benefit of the general reader. To understand what a rebreather is and how it works, it is useful to understand how a conventional open-circuit ("scuba") system works. The open-circuit system employs a compressed gas supply and a demand regulator from which the diver breathes. The exhaust gas is discarded in the form of bubbles with each breath.
A diver on the surface will normally metabolise between 0.7 and 1.5 litres of (surface pressure) oxygen per minute, although this figure can apparently range from 0.5 to 3 litres/min, and will depend very much upon the individual and work rate. An important point to note is that this rate of oxygen consumption will remain fairly constant once the diver is under water, and is irrespective of dive depth. For the following calculations, I'll try to keep things simple, so we will use an oxygen consumption rate of 1 litre per minute, which is actually reasonably typical. We will also assume that the diver is breathing at a rate (respiratory minute volume, or RMV) of 20 litres per minute, again reasonably typical.
At the surface, the 20 litres of air breathed per minute will contain about 4 litres of oxygen and 16 litres of nitrogen. From this air, our typical diver will metabolise just 1 litre of the oxygen in the mixture, and the remaining 19 litres – 95% of the total volume – are breathed out unused and effectively wasted.
We experience a pressure of approximately one bar from the overlying atmosphere when standing at sea level. Conveniently for our calculations, a 10-metre column of sea water also exerts a pressure of approximately one bar. Once underwater, the diver therefore experiences the combined pressure of the overlying column of water plus the overlying atmosphere. Thus, at a depth of 10 metres, the absolute pressure experienced by the diver is one bar of water pressure plus one bar of atmospheric pressure.
In order for the diver to be able to breathe under water, allowance needs to be made for the overlying pressure, or the divers lungs would quickly collapse. In an open-circuit diving system, the demand regulator reduces the high pressure in a diving cylinder to the same pressure as the diver's surroundings so that the diver's lungs do not have to work against the overlying water and atmospheric pressure. Incidentally, this overlying pressure of water is the reason that a diver's snorkel cannot be greater than around 40cm in length.
For each 10 metres of depth, the demand regulator will increase the pressure of gas delivered to the diver's lungs by one bar in order to compensate for the additional water pressure. If the RMV of the diver is 20 litres per minute, each additional bar of pressure corresponds to a further 20 litres of (atmospheric pressure) gas consumed per minute. Yet, as noted above, the rate of oxygen consumption is largely the same at all depths. Summarised in a table, it becomes clear just how wasteful the open-circuit system is as the depth of the dive increases:
|
Depth (m) |
Absolute Pressure (bar) |
Air Consumption (litres/min.) |
Air Wasted (litres/min) |
|
10 |
2 |
40 |
39 |
|
20 |
3 |
60 |
59 |
|
30 |
4 |
80 |
79 |
|
40 |
5 |
100 |
99 |
|
50 |
6 |
120 |
119 |
At a depth of, for example, 40 metres, we can see that the diver will breathe 100 litres of air per minute, metabolise 1 litre of oxygen and discard the remaining 99 litres of air – which still contained 19 litres of oxygen. Irrespective of whether the diver is using compressed air or a more exotic mixture of gases, such as a trimix, the diver on an open-circuit system will metabolise around 1 litre of oxygen per minute and literally blow off the rest.
To summarise:
- The absolute pressure experienced by a diver is a combination of the overlying atmosphere, plus the overlying column of water.
- Open circuit becomes increasingly wasteful the deeper the diver goes.
- The deeper you go, the more breathing gas you waste – and the less underwater time you have inside your cylinders.
- In terms of time spent underwater, the deeper you go, the less time you will have at the "sharp end".
5. Partial Pressure: Raising the Bar
Most people who know something about diving are likely to be aware of the potential problem of "nitrogen narcosis" during deeper dives, generally those below 30 metres. What is perhaps less widely known outside diving circles is that oxygen, a gas so vital to life, can become toxic at higher pressures.
5.1. Oxygen toxicity is a well document phenomenon and a quick Internet search will reveal a wealth of information, should the reader be curious. The toxicity of oxygen is determined both by the oxygen partial pressure [see below] and by the duration of exposure. Symptoms of oxygen toxicity can range from drowsiness, nausea, vertigo, tinnitus, muscular twitching and visual disturbances through to convulsions similar to an epileptic "grand mal". Convulsions underwater will result in a loss of consciousness and are very likely to result in death unless immediate help is available. They are therefore to be avoided at all costs.
Tests have shown that different individuals have markedly different tolerances to an elevated partial pressure of oxygen, that differences in the environment can change one's tolerance and that the same individual's tolerance can vary significantly on different days. People can also experience convulsions without having been aware of any precursor symptoms. No correlation has been found between increased oxygen tolerance and a diver's age, weight, fitness or a host of other characteristics. On the other hand, decreased tolerance is closely linked to elevated levels of carbon dioxide, cold temperatures and even immersion in water.
As already mentioned, oxygen toxicity is related both to the partial pressure of the oxygen being breathed and the duration of exposure. The term partial pressure of oxygen is often abbreviated as either ppO2 or PO2. This article will use the former abbreviation. It is important that the reader understands the concept of partial pressure otherwise much of what follows will make little sense.
The partial pressure of any gas is a numerical measure that is derived from the product of the absolute pressure of the gas and the fraction (or percentage) of the gas in a given mixture. Using diving terms, partial pressure is calculated using the formula:
partial pressure = absolute pressure x volume fraction of gas component
There are various caveats to this formula that are relevant in scientific calculations but the formula is sufficient for diving purposes and has the benefit of simplicity. The term "volume fraction of of gas component" refers to the fraction of the gas, in this case oxygen, in the overall mixture.
For air, and assuming an oxygen volume fraction of gas component of 0.21 (ie 21%), the ppO2 at various depths will be:
|
Depth (m) |
Absolute Pressure (bar) |
ppO2 (bar) |
|
0 |
1 |
0.21 |
|
10 |
2 |
0.42 |
|
30 |
4 |
0.84 |
|
50 |
6 |
1.26 |
|
70 |
8 |
1.68 |
The human body is tuned to exist at a ppO2 of 0.21 bar. If there is too little oxygen, we might get altitude sickness or black out (hypoxia). If there is too high a ppO2, we might experience oxygen toxicity. Tests on volunteers have established that the safe range of ppO2 goes from around 0.16 bar at the lower end of the scale to as high as 1.6 bar at the upper end of the scale. For example, the American organisation, the National Oceanic and Atmospheric Administration (NOAA) recommends a maximum single exposure of 45 minutes at 1.6 bar absolute pressure, of 120 minutes at 1.5 bar, of 150 minutes at 1.4 bar, of 180 minutes at 1.3 bar and of 210 minutes at 1.2 bar.
If we take a ppO2 of 1.3 bar as our safe limit, which is the recommended limit for the Inspiration rebreather, we can work backwards to find the maximum safe depth for diving on air as being:
= 1.3 / 0.21 = 6.19 bar absolute pressure
which equates to a depth under water of about 52 metres. This establishes the maximum safe depth for diving on air if the duration is expected to be 3 hours at depth, which is also the Inspiration's official limit. Of course, it is not a hard and fast depth since it is affected by the time at depth and some people suggest 1.4 bar as a safe limit, but it shows that at around 50 metres the average diver on air is likely to reach a maximum safe ppO2 limit. As an aside, a diver breathing 100% oxygen would experience a ppO2 of 1.3 bar at a depth of just 3 metres.
So how does a diver go deeper than 50 metres? The answer is simple: reduce the percentage of oxygen in the breathing mixture. For example, by reducing the percentage of oxygen in the breathing mixture to 10%, we see the following:
|
Depth (m) |
Absolute Pressure (bar) |
ppO2 (bar) |
|
0 |
1 |
0.1 |
|
10 |
2 |
0.2 |
|
30 |
4 |
0.4 |
|
50 |
6 |
0.6 |
|
70 |
8 |
0.8 |
|
100 |
11 |
1.1 |
|
120 |
13 |
1.3 |
|
140 |
15 |
1.5 |
We're now extended our safe depth to 120 metres. Of course, there are catches. Although we have addressed the issue of oxygen toxicity, there's still the small matter of nitrogen narcosis to be addressed. Nitrogen narcosis is discussed below and is addressed in a similar way to oxygen toxicity: by reducing the percentage of nitrogen in the breathing mix. What the reader might also have noticed is that in the above table the breathing mixture is hypoxic, ie the ppO2 is too low [below 0.16 bar], when the diver's depth is less than 6 metres. In open-circuit diving, this problem can be addressed by having two breathing mixtures: one for shallow water, eg air, and one for deep water.
Although the focus has so far been on oxygen toxicity, oxygen is also a potentially narcotic gas under pressure [see below].
5.2. Nitrogen narcosis is an altered state of mind caused by breathing nitrogen at a high partial pressure. The deeper a diver descends, the higher the partial pressure of nitrogen (and other gases) in his breathing mixture will be. For this reason, nitrogen narcosis is largely related to depth: the deeper a diver goes, the greater is the potential narcotic effect.
In fact, there is evidence that oxygen also plays a part in the narcotic effects of a gas mixture and the current trend is towards treating oxygen and nitrogen as equally narcotic. The term nitrogen narcosis is therefore not strictly accurate and it is consequently sometimes referred to as inert-gas narcosis, or simply narcosis.
As with oxygen toxicity, the effects of narcosis (both nitrogen and oxygen) vary between individuals and depending on conditions, but the symptoms can include emotional changes, eg euphoria or irrational fear, impaired mental function and impaired motor coordination. For the individual, there is no reliable method to predict the depth at which narcosis becomes noticeable or its severity, as the effect may vary from dive to dive (even on the same day). The individual may also not notice the onset of narcosis or be aware that he is "narced". Many studies have been made of the effects of narcosis and a common theme is that people who are so grossly impaired by serious narcosis that they are unable to perform even the most trivial of tests later harbour the belief that they did well – that is if they remember anything at all.
Some open-water divers seems to be quite relaxed about going to -60m on air, as long as the conditions are relatively stress-free, eg calm sea conditions and good visibility. Although some effects of narcosis are almost certain to be apparent by that depth, the experienced diver can often fight against the narcotic haze and continue with the dive. In situations where conditions are perceived to be more stressful or the task-load is higher than normal, outside distractions can make it more difficult to focus effectively on the task in hand. For the cave diver, who may be without a buddy, narcosis can have serious consequences. Opinions seem to vary about what is considered to be the maximum depth that a diver on compressed air can tolerate narcosis but going below m is generally considered to be into the highly risky zone. Of course, by this point the risks of oxygen toxicity on air will also be high. See http://www.divermag.com/nitrogen-narcosis-a-critical-conversation/ for an interesting analysis of narcosis.
5.3 Carbon Dioxide Narcosis. Carbon dioxide (CO2), which is a by-product of the body's metabolic processes, can be a significant threat to a diver's safety. It is not only an asphyxiant but is also a highly potent narcotic that is considerably more potent than either nitrogen or oxygen. An indication of its potency is that it can produce surgical levels of anaesthesia, with a very rapid onset, at sufficiently high concentrations. It has undesirable side effects that preclude its use as a general anaesthetic for humans but is commonly used to incapacitate animals prior to slaughter.
Increased CO2 in the bloodstream (hypercapnia) impairs physical, as well as mental, skills. Severe elevation of arterial CO2 can depress the level of awareness and prevent a diver from recognizing and reversing the process. Divers have become incapacitated and lost consciousness due to high arterial CO2 levels without any awareness of being in a life-threatening situation. As noted earlier, higher CO2 levels are linked to an increased susceptibility to oxygen toxicity and may also increase susceptibility to nitrogen narcosis. A table listing the effects of progressively higher percentages of breathed CO2 (at atmospheric pressure) can be found at http://www.analox.net/carbon-dioxide-dangers.php.
There is also evidence to show that the mechanism through which the human body controls CO2 levels in the bloodstream can be impeded when using a higher than normal partial pressure of oxygen, as is generally the case with rebreathers, leading to a build-up of CO2 without the usual increase in breathing rate. This is thought to be one reason why people may lose consciousness without ever having been aware of a life-threatening build-up of CO2 in the bloodstream.
For the rebreather diver, an elevated level of arterial CO2 is likely to arise from four main sources, two external and two internal. Firstly, the diver might re-breathe some of the exhaled CO2 as a result of the rebreather's scrubber mechanism [see below: section 6.2] failing to do its job effectively, which is often referred to as CO2 "breakthrough". Secondly, exhaled CO2 may be re-breathed because pockets remain within the breathing loop. Thirdly, CO2 can build up within the bloodstream as a result of high workload and, fourthly, it might remain in the bloodstream because of insufficient or inefficient breathing.
5.4. Gas Density. As the depth – and therefore pressure – of a dive increases, so does the density of the gases breathed by the diver. As we dive deeper, gas density becomes a significant factor affecting our ability to ventilate our lungs. In practical terms, the deeper we dive the harder we have to work to breathe, due, in part, to increased gas density. This is often referred to as the "work of breathing" (WOB). As well as requiring more effort, the higher gas density at depth means that we are also not able to move as much gas in and out of our lungs, no matter how hard we may try. The measure of how much air we can move in a specified period of time is often referred to as the "maximum voluntary ventilation" (MVV). Quoted figures seem to vary but suggest that at a depth of just 30m MVV capacity when breathing normal air is around 50% that at the surface, and at a depth of 100m is just 30% that at the surface. Increasing depth is not the only factor that may reduce breathing capacity, but this change in MVV alone is sufficient to ensure that our work capacity at depth is much less than at the surface.
The diver using a rebreather must move gases through the breathing loop by lung power alone. As the density of the breathing gas increases, this can become very hard work for the rebreather diver and, with increased depth, can be likened to breathing through a pipe of progressively diminishing size. An increased WOB and reduced MVV can potentially lead to an increase of retained CO2 in the bloodstream. If we cannot fully ventilate our lungs during a dive, CO2 can build up. Normally, as CO2 builds up our body responds by increasing the breathing rate and volume to expel it. However, a decreased MVV places a cap on how much gas we can physically move in and out of our lungs. The harder we work to breathe, the more CO2 we will generate, potentially trapping us in a downward spiral. In extreme cases it is quite possible to reach a point where attempts to reduce CO2 in our bloodstream through heavy panting can generate more CO2 than we are able to expel through the lungs.
The following table shows the gas density of five major gases found in air, at sea level pressure and a temperature of 20ºC:
|
Gas |
Density (grams/litre) |
|
Helium |
0.1664 |
|
Neon |
0.8385 |
|
Nitrogen |
1.1652 |
|
Oxygen |
1.3314 |
|
Argon |
1.6619 |
Note that Helium has a relative density that is only 14% that of nitrogen. This significantly reduces the WOB (and improves MVV) and is one of the main reasons that it is used in deep-diving breathing mixtures.
5.5. Breathing Mixtures. Non-air breathing mixtures usually come in three broad categories:
- Nitrox: As the name suggests, this is a mixture of nitrogen and oxygen. Although air would fit the bill as a nitrox, the name is often reserved for breathing gases where the ratio of nitrogen to oxygen is different from that found in air (although it is possible to find references to "normoxic nitrox" on the Internet). Generally, the oxygen portion is increased and the nitrogen portion is correspondingly reduced. An increased percentage of oxygen has the effect of reducing the safe working depth with regard to oxygen toxicity of the gas but the reduced percentage of nitrogen can help with decompression times.
- Trimix: This is a mixture
of three main components: helium, oxygen and nitrogen. If we want to
dive deeper than 50 metres we need to reduce the percentage of both
oxygen and nitrogen in the breathing mixture. Helium has very little
narcotic effect and, as noted above, gives significantly reduced
breathing resistance at depth. The main disadvantage of helium is
that it is relatively expensive, particularly for open-circuit
diving.
Conventionally, trimix is named by its oxygen percentage and helium percentage (and, rarely, also by its third component). Thus a trimix comprising 15% oxygen and 50% helium will be labelled as "trimix 15/50".
Dives below 100m generally need to reduce the percentage of oxygen and nitrogen further, so trimix ratios like 10/70 are often used deeper down. Włodek used a 10/70 trimix in his rebreather for deeper dives.
- Heliox: This is a mixture of only helium and oxygen. It is generally reserved for deep saturation diving and produces the distinctive "Mickey Mouse" voice when breathed. It is more expensive than trimix and it can induce tremors at depth.
To summarise:
- Oxygen toxicity and nitrogen/oxygen narcosis will limit the depth at which a diver can go on a given gas mixture.
- Carbon dioxide is a potent narcotic that can also increase susceptibility to oxygen toxicity and nitrogen/oxygen narcosis.
- The generally accepted safe ppO2 upper limit is somewhere around 1.3-1.4 bar, and above 1.6 bar is considered to be dangerous.
- Increased gas density at depth means that the diver must work harder to breathe. For the rebreather diver, this can be even more of a problem. Increased WOB and reduced MVV can lead to CO2 retention.
- In order to dive deeper than about 50 metres, the diver must reduce the percentages of oxygen and nitrogen in the breathing gas below those found in air. For cave diving, that normally means some variation of a trimix.
6. The Rebreather
As already mentioned, Włodek bought a Buddy Inspiration rebreather at the end of 2002. His motivation for doing so was that the new equipment would allow him to push the limits of cave-diving exploration, much as he'd long been doing in conventional cave exploration. Plus, the rebreather is a gadget par excellence, and Włodek was always attracted to gadgets. Then there are all the other bits and pieces that the diver needs: dry suit, extra cylinders, demand regulators, dive computers, rebreather modifications, lights, hoses, harnesses. The list is potentially endless.
So what is a rebreather? There are three basic types of rebreathers currently in use: the oxygen rebreather, semi-closed rebreather, and closed-circuit rebreather. The Buddy Inspiration (now renamed Inspiration Classic), which is the focus of this article, is a closed-circuit rebreather (CCR). As the name suggests, the closed-circuit rebreather recirculates exhaled gases within the apparatus, ie inside a closed breathing circuit, rather than expelling them as bubbles, so that the diver can breathe them again and again. As has already been demonstrated, the open-circuit system is very wasteful, particularly at greater depths. Recirculating the exhaled gases is the key to the rebreather's efficiency.
A simplified schematic diagram of a generic closed-circuit rebreather can be found at http://en.wikipedia.org/wiki/File:Fully-closed_circuit_rebreather.PNG The simplified CCR exhibits the following key components:
- Breathing gas (or "diluent") cylinder
- Oxygen cylinder
- Carbon dioxide scrubber
- Counterlung
- Manual valves: diluent and oxygen
- Automated oxygen valve
- Oxygen sensors (or "oxygen cells")
- Oxygen controller
- One-way valves
- Mouthpiece.
A more detailed schematic of the Inspiration Classic can be found at http://www.apdiving.com/downloads/downloads/Inspiration (Classic) Schematic.pdf
A quick note on the components:
- The Inspiration cylinders have a 3-litre capacity and a fill capacity of around 200 bar for oxygen and 232 bar for the diluent. The diluent gas can be air, trimix or heliox.
- The carbon dioxide scrubber is a cylinder packed with granules of a CO2 absorbent material, which is designed to remove CO2 from the exhaled breath. The Inspiration's scrubber is rated for 3 hours when used in accordance with a strictly defined set of parameters. Włodek believed that he could eke 5 hours from it. [In fairness, he was was not alone in this belief.] A more detailed description of the Inspiration's scrubber mechanism is given below.
- The counterlung is a bag (two bags in the case of the Inspiration) that allow the diver to breathe. Were there no counterlungs, the exhaled breath would have to stay within the confines of a rigid pipe system, rendering breathing impossible. The medium-size counterlungs on the Inspiration each have a maximum capacity of 5.7 litres.
- The automated oxygen valve is activated by an electric solenoid.
- The oxygen cells read the ppO2 in the breathing loop. The Inspiration has three sensors so as to provide a level of redundancy, should one cell fail. A good cell should give an accurate reading within six seconds.
- The oxygen controller is a computer that takes readings from the oxygen cells and, if necessary, opens the oxygen valve until the required ppO2 is reached at the oxygen cells. The Inspiration has two independent oxygen controllers.
- The one-way valves ensure that the gas circulates the correct way in the breathing loop.
There are many excellent articles to be found on the Internet that go into considerable detail about the internal workings of the CCR and this article cannot possibly seek to replicate the considerable body of work already available. I will therefore focus on those rebreather topics that I think are relevant to Włodek's accident.
6.1. Diluent: The diluent is the main breathing gas used in a CCR and, for reasons that will be discussed later, will always contain a certain percentage of oxygen. On a rebreather the diluent is usually either air or a trimix (or, more rarely, heliox). A critical requirement of a diluent is that it should be able to sustain life at the maximum dive depth. If the ppO2 of the diluent is insufficient, oxygen can always be added but oxygen cannot quickly be removed from a potentially toxic diluent. Thus, air is a suitable diluent down to around 50 metres depth, since its ppO2 will be within safe limits at 1.26 bar. Beyond 50 metres, a suitable trimix will normally be necessary as a diluent.
6.2. Carbon Dioxide Scrubber: As mentioned, this is a container that is filled with a material that absorbs CO2 from the exhaled breath and is one of the most critical components in the rebreather.
The design of CO2 scrubbers in general seems to be as much of an art as a science and their success or failure in operation can be the result of sometimes subtle but critical processes and interactions. In order to ensure the successful operation of the scrubber – and with it the safety of the diver – the Inspiration's manufacturer is very prescriptive about how it should be filled and with what specification of CO2 absorbent.
The Inspiration rebreather has received a CE certification, and was the first commercial rebreather to do so. Part of the certification process involved independent testing carried out at the UK Ministry of Defence Research Establishment, Alverstoke. The Inspiration's scrubber duration was rated to be 3 hours in the following circumstances: a water temperature of 4 degrees Celcius; a simulated breathing rate (RMV) of 40 litres per minute (lpm); a CO2 production rate of 1.6 lpm; a constant depth of 40 metres; and a maximum allowed CO2 breakthrough level of 0.5%. The tests used only one type of CO2 absorbent: 8-12 mesh Sofnolime 797, manufactured by a British company, Molecular Products Ltd. At the time of writing, 8-12 mesh Sofnolime 797 is the only absorbent that is officially recommended for use in an Inspiration rebreather. The absorbent contains granules between 1mm and 2.5mm in size that have a triangular cross section, enabling a close packing density. The close packing and small granule size are said to provide the optimum balance between scrubber efficiency and an acceptable WOB.
Apart from choosing a suitable absorbent, the main factors that will affect the duration of the Inspiration's CO2 scrubber are: the diver's workload (and therefore CO2 production); the water temperature; and the depth of operation. While it is relatively straightforward to calculate one's personal CO2 production rate, the effect of the two other factors is difficult to predict. Consequently, for very deep dives the rebreather diver needs to be particularly careful to follow the recommended procedure. To quote a press release from Ambient Pressure Diving, the Inspiration's manufacturer, (http://www.xray-mag.com/content/important-notice-ap-diving-various-co2-absorbents-are-sold-diving ):
Why does the granule size matter?
The
smaller the granule, the larger the surface area of sodalime in contact
with the incoming gas, so the CO2 is absorbed within a
shorter bed length; i.e. the "reaction zone" is shorter with small
granule materials.
CO2 comes through the scrubber when
the front edge of the reaction zone reaches the far end of the scrubber.
The larger the granule size, the longer the reaction zone, the
earlier CO2 comes through.
Depth has an
incredibly detrimental effect on scrubber duration and we have seen in
our test rig extremely short durations with coarse granule absorbents.[My
emphasis. Comment: Strictly speaking, it appears to be gas density,
rather than depth, that is the determining factor at work here, although
the two are normally closely related.]
6.3. Regulating ppO2. An Inspiration rebreather contains two gas cylinders: one containing the diluent, and the other containing pure oxygen. The rebreather's breathing loop is filled with diluent and a monitoring system automatically adds oxygen from the second cylinder so as to maintain a pre-set ppO2 level, known as a "setpoint". Assuming a ppO2 setpoint of 1.3 bar is being used, the percentage of oxygen in the breathing loop will reduce as depth increases:
|
Depth (m) |
Absolute Pressure (bar) |
%age Oxygen |
|
30 |
4 |
32.5% |
|
50 |
6 |
21.7% |
|
70 |
8 |
16.3% |
|
100 |
11 |
11.8% |
|
120 |
13 |
10.0% |
The table begins at 30 metres because the Inspiration rebreather, for a variety of technical reasons, will generally be used with a ppO2 setpoint of 0.7 bar for the first 20-30 metres of a dive – and around 1.3 bar thereafter. Note that between 30-50 metres, the percentage of oxygen shown in the table above is actually higher than that found in air. The foremost reason for first using a low setpoint is that it is simply not possible to achieve a ppO2 of 1.3 bar while at the surface. The conventional recommendation is that the high setpoint should then be used deeper down so that the higher oxygen concentration arising from the high setpoint effectively displaces a portion of the nitrogen that would otherwise occur in the breathing mixture, thereby helping with decompression times during the ascent. The main objection to this strategy is that the 1.3-bar setpoint, while below the accepted safe maximum level, is edging a bit too close for some tastes. While this recommendation has some merit when an air diluent is used, its adoption when using a trimix diluent with a low nitrogen content is less clear cut. There is an alternative strategy that is also used by rebreather divers, which is to use a low (0.7 bar) setpoint during the entire descent phase and then (optionally) switch to the high setpoint when at the bottom. This approach has the benefit of keeping the diver further away from the critical 1.6 bar alarm point during the descent, thus allowing the diver greater headroom for any ppO2 "spikes" [see below] above the setpoint that might occur.
As the diver descends and the pressure increases, pressure compensation is required to allow the diver to breathe, just as it is with an open-circuit system. On a rebreather this is achieved by adding further diluent to the breathing loop, and can be accomplished either via an automatic diluent valve (ADV) or through a manually-activated valve (MAV). If the operation is manual, the amount added and frequency of addition will be determined by the speed of the descent, the desire to control the ppO2 and what is most comfortable for the diver's (work of) breathing. Generally, small and frequent injections of diluent will be preferable.
In practice, since the diluent will always contain a percentage of oxygen, adding diluent may slightly alter the ppO2 in the breathing loop. At the same time, the diver will continue to remove one litre (or thereabouts) of oxygen per minute from the gas he is breathing, thereby reducing the ppO2 in the breathing loop. This gives rise to three possible situations during a descent:
- The diver metabolises more oxygen than was provided in the fresh diluent. If so, the rebreather should automatically add oxygen to the breathing loop to bring the ppO2 back up to its setpoint.
- The diver metabolises the same amount of oxygen as was provided in the fresh diluent, Since they are both in equilibrium, the rebreather has no need to add further oxygen, and the ppO2 will remain unchanged .
- The diver metabolises less oxygen than was provided in the fresh diluent. The rebreather will again have no need to add further oxygen but the ppO2 will rise above its setpoint. For this reason, the rebreather diver needs to be careful not to descend too quickly, since there is a danger that the unused oxygen will cause the ppO2 level to rise faster than can be accommodated by the diver's metabolism, leading to a so-called ppO2 "spike" above the setpoint.
Should the ppO2 rise above its setpoint, all is not lost. If the amount is minimally over the setpoint, the diver has the option to cease or slow the descent and wait until his metabolism of oxygen brings the level down sufficiently. If the diver is descending using a low setpoint, eg 0.7 bar, there is more leeway and the ppO2 can rise significantly above the setpoint before the diver needs to consider taking any kind of remedial action. Of course, all this depends upon the diver continually monitoring the ppO2 level on the display of his oxygen controller. Should the diver be otherwise engaged or the rise in ppO2 be unexpectedly rapid, monitoring might not occur sufficiently often, so the Inspiration is equipped with an alarm which will sound when the ppO2.rises to 1.6 bar. [As an aside, cave divers sometimes experience near-zero visibility in caves making such regular visual monitoring very difficult.]
If an alarm sounds, the diver quickly needs to ascertain the cause of the alarm and, where possible, take appropriate action. On the Inspiration, an alarm can sound for a variety of reasons, such as a faulty oxygen sensor being detected, as well as the ppO2 level exceeding the safety threshold of 1.6 bar. A "diluent flush" is usually the diver's preferred method of dealing with a high-ppO2 alarm.
Performing a diluent flush is a fundamental part of a rebreather diver's training and involves purging the breathing loop of the potentially toxic gas mixture with fresh diluent. It is accomplished by manually opening the diluent valve for about 10 seconds while simultaneously opening a purge valve on a counterlung. This will effectively reset the ppO2 of the breathing loop to that of the diluent.
6.4. Bailout. A major limitation of the rebreather is what does the diver do if the system suffers a serious malfunction while being used? The answer is to abort the dive, known in the jargon as a "bailout" [sometimes "bail out"]. All well and good, but clearly the diver must still breathe while getting back to the surface. The official bailout procedure of the Inspiration is therefore that the diver moves from breathing on the closed-circuit breathing loop and switches to breathing on open circuit directly from the diluent bottle through an alternative mouthpiece/demand regulator [and is another reason why the diluent mix must sustain life at the maximum depth.] This approach has some serious limitations. Firstly, at depth, open circuit is very wasteful – and the diluent cylinder has a capacity of only 3 litres, giving very little margin for safety. For example, using our previous example RMV of 20 litres/min, at a depth of -80m a full diluent cylinder will be good for just 3 minutes, giving no time for decompression. For open-water diving this might be just about tolerable in limited circumstances but is absolutely unacceptable for cave diving. Secondly, many divers argue that if the rebreather has malfunctioned, the diver should get off the rebreather system immediately and cannot rely on it any further to get out of trouble. For cave diving, where duplication of critical system elements is the norm, these are unacceptable limitations. The prudent cave diver will therefore need to add external cylinders to beef up the rebreather's bailout capabilities and provide sufficient breathing gas, on open circuit, for the diver to return to the surface, including decompression stops. This adds to the weight and complexity of an already complex set of equipment.
A conventional bailout requires the switching of mouthpieces. Switching mouthpieces underwater is not a difficult procedure but can be prone to error, particularly in stressful conditions and/or poor visibility. In situations where the diver is experiencing a severely elevated level of CO2, the rapidity and depth of breathing might be so great that there will be a very great reluctance to remove the mouthpiece for even the briefest of moments. In practice, the closed-circuit mouthpiece also needs to be switched off before removing it otherwise the system might flood, further complicating the process. To overcome these limitations, Włodek added a modification to his Inspiration so that a bailout valve was directly incorporated into the Inspiration's breathing loop mouthpiece. The valve was manufactured by a fellow Pole, Filip Królak. On the valve's face there is a large switch. When the switch is in a horizontal position, the diver is using the closed (rebreather) circuit. When the switch is in a vertical position, the breathing loop is closed off and a demand regulator is switched on. With just a quarter turn of the switch, Włodek was able to switch between closed- and open-circuit modes. A description of the valve can be found at http://www.therebreathersite.nl/05_Reviews/review_oc_cc_mouthpiece.htm [The warning at the top of the page is interesting and suggests that there were serious usability problems with this particular unit. However, people I have personally spoken to were positive about it.]
The rebreather clearly addresses the wastefulness of the open circuit system but at a price of increased complexity. With an increase in complexity arguably comes an accompanying increase in risk. Add to this that the rebreather can extend the ability of the cave diver to push the limits of exploration, and it's clear that the explorer's metaphorical tightrope has become significantly thinner. Proponents of the rebreather have long argued that the additional risks can largely be mitigated by strict adherence to procedures and a rigid maintenance schedule. Well, maybe…
7. The Accident
By 2005, Włodek had become one of Poland's leading cave divers. He had racked up a significant number of cave-diving excursions both abroad and within Poland since his rookie days back in August 2001 and had recorded details of them on his Deep and High web site. In July 2002, he had joined up with the OUCC Tormenta 2002 expedition to the Picos and, together with Wiktor Bolek, had (unsuccessfully) attempted to link the C4 sump with 2/7. In 2003 he made over 30 dives and had reached a maximum depth of -102.7 metres on his rebreather. 2004 saw Włodek dive close to -100 metres on at least three occasions. May 2004 saw the tragic death of his cave-diving mentor and top-tier Polish cave diver, Wiktor Bolek, apparently of natural causes, while diving in a flooded quarry. It was Wiktor who had been the driving force behind the exploration of Izbucul Tauz and Włodek took up the reins in Wiktor's stead, organising trips in August and September 2004 and again in January 2005,
The January 2005 expedition to Izbucul Tauz
is interesting not for what was found but for what was to happen three
months later. A summary (in Polish) can be found on the "Deep and High"
site at
http://www.deepnhigh.pl/Włodek/Deep_+_High-_News/content_064.html.
The expedition left Poland on 12 January 2005, with one contingent of
people, including Włodek, leaving from the city of Wrocław and some
others leaving from Warsaw. It appears that one of the Warsaw members
picked up at least one freshly-filled Inspiration diluent cylinder from
a professional filling service in Warsaw that Włodek regularly used. The
label on the cylinder states that it was filled on 12.01.05 and
contained 10.3% O2, 73.9% He and 15.8% N2.
 |
 |
|
| Trimix cylinder used on the January 2005 dives | Trimix cylinder used on the April 2005 dive |
Włodek undertook just one dive, of duration 2 ½ hours and went to a depth of -85m.
For the next two and a half months, Włodek seems to have done no further diving. Then, on 4 April 2005, he joined a small team organised by another Wrocław cave diver and headed off to the pretty town of Bourg Saint Andéol in the Ardèche department of France. This was very much at the tourist end of the spectrum, since the caves at Bourg Saint Andéol were already being explored by French divers.
At around 21:00 on 5 April Włodek dived for around 80 minutes to a maximum depth of 9.4 metres in what is very likely to have been the Goul de la Tannerie cave. This dive was recorded on one of his dive computers.

The next cave that Włodek chose to dive in was Goul du Pont, which is situated just a few hundred metres from the Goul de la Tannerie. http://plongeesout.com/sites/raba/ardeche/goul%20pont.htm The cave is situated within the boundaries of Bourg Saint Andéol and is to be found under a viaduct of the SNCF railway [Google Maps]. A quick look at the description of the cave shows a superb diving environment with easy access, spacious passages of splendidly clear water http://vimeo.com/18527849 http://www.dailymotion.com/video/x18fsx_goul110_sport (NB videos: both recommended) http://alexandrefox.over-blog.com/album-1838147.html, an enticing vertical pitch of 30m http://plongeesout.com/sites/raba/ardeche/goul%20pont%20photo08%20grand.JPG http://plongeesout.com/sites/raba/ardeche/goul%20pont%20photo09%20grand.JPG and an explored depth, at the time, of -178m (since pushed to -185m). What better place than to improve on his personal depth record of -102.7m, recorded back in 2003! [Update: The depth limit was pushed to -192m on 15 June 2013 by a Polish diver, Krzysztof Starnawski. An excellent video of the record-breaking dive can be found at http://vimeo.com/68868623 ]
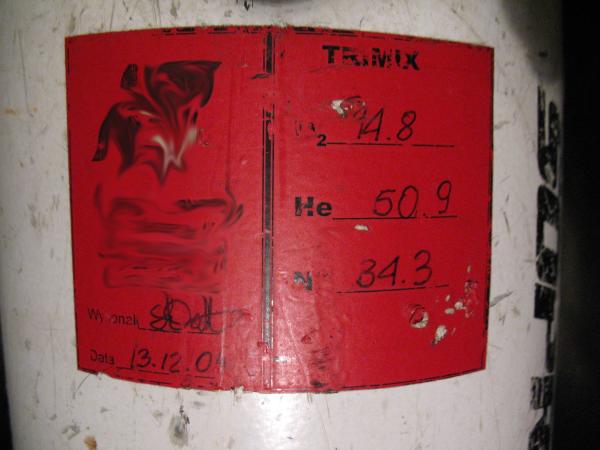
Prior to the dive, it is reported that Włodek had some problems with the rebreather's oxygen sensors being affected by dampness. This is very likely to have been due to the residual moisture left inside the rebreather from the previous evening's dive and the fact that overnight temperatures in early April are likely to have been cool, hampering the evaporation of residual moisture within the system. Nevertheless, the problem does not seem to have been insurmountable and shortly after 09:30 on 6 April 2005, Włodek entered the sump pool and started to run his pre-dive checks. Along with his rebreather, he was carrying two side-mounted 10-litre dive cylinders, one with a 40% nitrox mix and the other with a 15/50 trimix that showed a fill date of 13.12.04.
By about 09:55 he was ready to go. These are the last photos taken of Włodek alive:
 |
 |
 |
With a call-out time set at 15:00, he started his dive.
By 15:00 he had not returned and the surface party decided to try to see for themselves if anything could be done, carrying out two dives to a maximum depth of -70m, but to no avail. With all reasonable hope gone, the rescue services were alerted for what was by then certain to be a body retrieval.
The next day, the French rescue party located Włodek's body at a depth of -105m – close to the bottom of the 30m pitch – with the mouthpiece out of his mouth, and began the grim process of retrieval. Further details of the rescue can be found at http://speleo-secours-francais.com/index.php?option=com_content&view=article&id=117:20050406gouldupont07
The accident was discussed in some detail on a (French language) forum, and can be found at http://www.plongeesout.com/causette/archive_mars_2007/affiche4c7c.html?message=5302. A first-hand summary (in English) of the rescue can also be found at http://www.rebreatherworld.com/rebreather-accidents-incidents/364-goul-du-pont-polish-diver-inspiration.html. Both contain a wealth of important information that will be referred to during my analysis of the accident.
A brief summary of the accident can also be found at http://www.plongeesout.com/accidents/accidents%20ps%20france.htm.
The French police tried to impound all of Włodek's belongings. For reasons that remain unclear, Włodek's diving colleagues did not hand over some of his possessions, including two spare Inspiration (3-litre) bottles – one diluent and one oxygen – that Włodek had brought with him. These withheld items returned to Poland, unexamined by the French police. This has a further twist, which will be discussed later.
Because of bureaucratic problems, Włodek's body was not repatriated until over a month after his death. He was finally buried in his home town of Wrocław on 14 May 2005. http://www.oucc.org.uk/dtt/vol15/dtt15_09.htm
8. The Official Report
As might be expected following such a death on French territory, the authorities launched an investigation into what happened. The examining judge in charge of the case then commissioned an expert report from an experienced French diver, which was completed in November 2005.
The report runs to 13 pages and examines three pieces of equipment provided to its author:
- the Inspiration rebreather;
- a Delta P VR3 dive computer; and
- an Uwatec Aladin Pro Ultra dive computer.
Perhaps surprisingly, the French authorities had decided not to retain the 10-litre side-mounted external cylinders that Włodek used and had returned them to Poland together with his body. The reason for this is unclear from official documents I could find but Frédéric Badier's account at "Rebreather World" states that "Both cylinders were fully operationnal and untouched (2nd stage in position)." [2nd stage refers to the demand regulators attached to the cylinders. "In position" suggests that they were still secured to the cylinders, probably by rubber loops.] On the other hand, as will be seen, the author of the official report into Włodek's death was aware of the cylinders' existence but appears to have been unaware that they were found to be untouched, since he postulated the use of one in his hypothetical accident scenario.
It is neither possible nor sensible to provide a full translation of the report, so I'll concentrate on what I believe are the important points. What follows is a summary of what was written, complete with the original paragraph numbers, together with comments/clarifications in italics where appropriate.
Para. 3.31 Measurement of cylinder pressures
Diluent: 132 bar. The author comments that he thinks the accident likely occurred quickly when, or just before, Włodek reached -107m. This cylinder pressure is abnormally low for a closed-circuit dive. This suggests that Włodek breathed from the cylinder on open circuit prior to the accident. Other facts confirm this hypothesis.
Oxygen: 10 bar The pressure is excessively low. This could result from a gas leak after the accident during which time the rebreather continued to inject gas, or possibly a leak caused by the rescuers. [Comment: This is effectively an empty cylinder, which would seem to be potentially a big deal. For reasons that are unclear, the empty oxygen cylinder is rejected as being a possible cause of the accident, but the author offers no clear evidence to show why he believes this to be so.]
Para. 3.33 Analysis of cylinder contents
Diluent cylinder: 21.3% Oxygen, 4.8% Helium
Affixed to the cylinder is a red label, covered with some white tape.
The red label indicates that the contents should be trimix 10/70.[Comment:
A 10/70 trimix will contain about 10% oxygen and 70% helium. The actual
mixture was dangerously incorrect for such a deep dive. The significance
of the white tape is unclear. Unfortunately, the author does not record
the fill-date that would have been shown on the label and neither does
he provide a photograph of it in his report. As will be seen, this is a
regrettable omission, given how critical the mixture was to any
investigation of the accident.]
Oxygen cylinder: 100% Oxygen
Para. 3.34 Examination of mouthpiece
The bailout valve was not an original fitting. The demand regulator was an Eisberg Sepadiver K96. The large switch was found to be in the open circuit (vertical) position. The author states that the modification was not the cause of the accident. [Comment: As will be discussed later, the post from Frédéric Badier says that the rescuers "closed" the mouthpiece before moving the body. Therefore it is not clear whether the position of the switch described in the official report is how the rescuers originally found the mouthpiece. There is evidence that the rebreather had been partially dismantled by the rescuers and was not given to the expert witness in the exact state as it had been when it came out of the water. It is therefore possible – and, indeed, sensible – that the bailout valve could have been returned to its original position once the rebreather was on dry land. If one of the original rescuers is reading this article, clarification of this point would be very helpful.]
Para 3.342 The counterlungs
These were not as originally supplied and were modified from the standard to provide an additional inflation point on each counterlung: one for diluent and one for oxygen. The author states that they could have allowed inflation of the counterlungs from Włodek's external tanks. The author states that modification was not the cause of the accident. The counterlungs were not flooded and contained only a limited quantity of water consistent with normal use. [Comment: See below under the heading Para 3.347 regarding the possibility that the rebreather had been partially dismantled by the rescuers.]
Para 3.345 Oxygen controller displays
These were both switched off at the power switch, probably by the police. The battery levels were 2.34V and 3.45V [should have been 6V]. Unable to recover any settings because the units would reset once fresh batteries were installed.
Para 3.347 Carbon dioxide scrubber
An electrical apparatus, not original to the rebreather, was connected within the lid of the scrubber to the oxygen cells and relayed information on the quality of the breathing mixture to a head-up display located on the mouthpiece.
The granules appeared to be fresh but the granule size was outside of the recommended specification at 3.5mm [should have been 1-2.5mm]. The weight of the fill was found to be 2.65kg, which is within normal limits and the material was not saturated with water. [Comment: This is a questionable observation. The weight for a fill using the recommended material, Sofnolime 797, should be around 2.45kg when dry. The dry fill weight of the absorbent actually used was not known.] The author suggests that the use of a non-recommended granule size could have affected the efficiency of the CO2 scrubber. [Comment. As far as can be ascertained, Włodek used an absorbent produced by a Polish chemical company, Synthos Dwory, from the town of Oświęcim. No doubt it was considerably cheaper than Sofnolime 797. Włodek also seemed to have suggested to diving colleagues that it performed better in tests than Sofnolime 797, although which tests he was referring to is not known. A specification for the product, dated 2007, states that the granules are formed from a cylindrical extrudate between 2.8mm and 3.5mm in diameter. The increased granule size and relatively poor packing density of the cylindrical granules represent a potentially significant degradation in the performance of the rebreather's CO2 scrubber. The reported lack of saturation would suggest that the rebreather had not flooded. However, this is called into question by a comment of Frédéric Badier on the French forum, [the original French text of quotations may also be found in appendix B]:
At 2005-04-08 20:07:41, Frédéric Badier
states:
The rebreather was flooded including the
cell compartment which can be explained by the
mouthpiece and Iong immersion of the rebreather in such conditions
(interpretation)] [My emphasis.]
Later, at 2005-04-12 18:25:47, Xavier
Méniscus states:
The seal and spacer were in place, when we
removed the buddy.
And at 2005-04-12 18:33:53, Frédéric Badier
confirms this point:
The seal and spacer were in place, we
checked.
This tells us that the rescuers knew (at least) two things: the rebreather was flooded and the seal and spacer (of the scrubber) were in place. In order to know the latter, they would have had to dismantle the head of the scrubber unit. In performing this task they would have seen that the unit was flooded but this action would have drained water from the rebreather's cell compartment – and possibly from the whole scrubber assembly. Fundamentally, this tells us that the rebreather was at least partially dismantled and examined by the rescuers before the official examination took place. If, as reported, the rebreather had been flooded, the CO2 absorbent would have become saturated. It therefore suggests that the expert witness's conclusion that the absorbent had not been saturated with water – possibly based solely on the measured weight of an unknown brand of absorbent – was incorrect.
While it was not known at the time whether the French authorities would launch a formal investigation into the accident, this was always a possibility. The fact that the expert witness appears to have been unaware that the rebreather had been flooded (and dismantled) suggests a failure to pass on critical information to the next stage of the investigation.]
Para 3.349 Oxygen cells
No faults found. Correctly identified 20.9% of oxygen in air.
Para 3.350 Oxygen solenoid
No faults found.
Para 3.41 VR3 dive computer
The author notes that it is possible to connect the VR3 to an Inspiration rebreather, so as to give an independent ppO2 reading, but that Włodek did not have the option installed.
Serial no: 3FA4F6595F2A743D
List of dive gases
Nitrox 99 max oper. depth 6m
Nitrox 40 max oper. depth 30m
Trimix 15/50 max oper. depth 97m
Trimix 10/70 max oper. depth 90m
Decompression settings: closed
circuit
ppO2 = 0.75 bar
diluent = trimix 10/70
Time of immersion: 09:13
Date: 6 April 2005
Maximum depth 107m
Dive duration 3091 minutes [51 hrs 31 mins]
For technical reasons, it was not possible to
download the dive profile from the VR3.
[Comment: The
decompression ppO2 setting of 0.75 bar is less commonly used for deeper
dives and, if correct, means that Włodek was running his rebreather on
the low setpoint. The maximum operating depth of the 15/50 trimix is
specified as 97m. This equates to a ppO2 of 1.6, which would probably be
acceptable as a bailout mixture.]
Para 3.42 Uwatec Aladin Pro Ultra dive computer
This was not configured for the use of any trimix. It contained one configuration: for a gas containing 22% oxygen. The author speculates that it was a backup computer in case of failure of the VR3.
It contained a record of a dive on 5 April 2005 (the day prior to the accident) of duration 83 minutes and depth 9.4 metres. It held no information relating to the dive on 6 April, which the author could not explain. [Comment: Very likely the Goul de la Tannerie http://www.plongeesout.com/sites/raba/ardeche/goul%20tannerie.htm]
Para. 3.5 Causes of the Accident
A translation of this section is reproduced in full. The original French text may be found in appendix A.
The evidence obtained during our [forensic] examination does not show evidence of a rebreather malfunction causing the diving accident.
However the mixture error in the composition of the rebreather is the cause of the accident.
This error is all the more deadly as during the descent the diver had to breathe 15/50 trimix from the beginning of the dive and to finish, in the deep exploration, on 10/70 trimix. Indeed, this mixture, being richest in helium (70%), is only 20% nitrogen, and should eliminate the problems of narcosis. Yet if he follows this procedure when, at a depth of around 80m to 90m, he injects air instead of a 15/50 trimix mixture, the narcotic effect of the nitrogen (nitrogen narcosis) is immediate. Rebreather divers are more susceptible to narcosis because ppO2 regulation, by being lower than that obtained in open circuit, leads to a far higher ppN2.
So for these reasons the manufacturer of the rebreather limits dives on air to 50m; not only because of nitrogen intoxication (N2) but also that [intoxication] of oxygen which could also occur. Furthermore as the Buddy rebreather works with oxygen values understood to be between 0.75 bar (low setpoint) and 1.6 bar (high setpoint), beyond 50m the electronic management of the rebreather cannot, maintain the ppO2 in this range because of the increase of the ambient pressure.
Thus, beyond 50m the diver must use a trimix (mixture) or heliox.
Moreover, this is associated with a very rapid increase in ppO2 in the loop and, in accordance with Dalton's law, is much higher than the 1.6 bar allowed by the machine.
As the diver continues to descend on air, the ppO2 does not stop increasing [continues to increase?] proportionally with the ambient pressure, and the ppO2 of injection of the mixture exceeds the critical value of oxygen (1.6 bar) acceptable to the rebreather and the alarms trigger (audible and visual).
Mr. Szymanowski, thanks to these alarms, sees
the problem but analyses it as a malfunction of the solenoid valve,
leading to hyperoxia. In that case, the recommended procedure is the
following:
– Look at the display to judge if the ppO2 is
climbing quickly or if it results from a spike caused by too fast a
descent.
– If it continues to climb, close the oxygen bottle
and reduce the ppO2 by flushing the loop with the diluent inflator.
– After flushing, breathe and reopen the O2 bottle while watching
the ppO2. If it climbs once more, the solenoid is stuck open, so close
the oxygen bottle.
– To continue using the rebreather, open
and close the oxygen valve for brief periods while checking the supply
of O2. Although this is not very practical, the rebreather can be used
as long as necessary, but the solution is to use the backup bottles in
open circuit (bail out).
Mr. Szymanowski applies this procedure. This manoeuvre remains ineffective, because the ppO2 of the injected diluent is greater than that allowed by the machine. Consequently, the victim can only switch the quarter-turn valve, the Eisberg 96 K mouthpiece, to open circuit. This is what he does (mouthpiece to bail out valve position) but the bottle feeding it is not adapted to the advancing depth because it is very narcotic and hyperoxic.
Although it is customary to dive alone underground, Mr. Szymanowsky could have avoided the accident if he were accompanied by a scuba diver to provide him a gas mixture appropriate to the depth. [Comment: Given that the report was written for the French court, the suggestion that Włodek "could have avoided the accident if he were accompanied by a scuba diver" is rather contentious, to say the least.]
9. Analysis of French Report
Some aspects of the accident are reasonably established facts:
-
Włodek died of drowning after the mouthpiece left his mouth.
-
The label on the rebreather's diluent cylinder indicated that it should have contained a 10/70 trimix.
-
The dliuent cylinder did not contain a 10/70 trimix. The composition of the gas was 21.3% oxygen and 4.8% helium. A reasonable assumption is that the rest (73.9%) is nitrogen, although the report does not confirm this.
-
The cylinder's pressure was measured to be 132 bar after the accident.
-
The oxygen bottle contained 100% oxygen at a pressure of only 10 bar after the accident.
-
Włodek was found at a depth of -105m and his VR3 dive computer recorded a maximum depth of -107m for the dive.
-
Włodek carried two external 10-litre cylinders: one containing 15/50 trimix and the other 40% nitrox. Neither appears to have been used.
The report suggests that the empty oxygen
cylinder in no way contributed to the accident, and speculates that some
kind of leakage occurred after the accident. Unfortunately, the author
offers no evidence to support this hypothesis. Nevertheless, I think he
is correct. On the
French forum, Xavier Méniscus reported [at 2005-04-11 18:49:16]
that, when he first found Włodek (at a depth of -105m), the oxygen
cylinder still showed gas pressure when he tested the inflator, although
he was unable to turn the body to see the pressure gauge. The cylinder
was left open for a further day at a depth of -77m, by which time it had
become almost fully discharged. The pressure loss seems to have occurred
during the time of the rescue and is described by Frédéric Badier in his
post at "Rebreather
World":
"From -105m , the body was lift up to 80m (up to
the entrance of the horizontal gallerie) after closing the
mouthpiece. During the ascent, the rescue diver listened the
buddy alarm and the O2 injection. The body was left until the next day
at this depth, the rebreather control was left on with the cylinders
open." [My emphasis.]
In theory, the behaviour observed is
broadly to be expected. As the diver ascends, the pressure – and
therefore the ppO2 – in the breathing loop will fall, eventually causing
the rebreather to inject oxygen into the breathing loop in order to
maintain the ppO2 at its setpoint. As will be shown later, when Włodek
was first found the ppO2 shown on the rebreather's (slave) oxygen
controller was around 0.93 bar and the setpoint was showing 0.7 bar. We
would therefore not expect the solenoid to have opened until the ppO2 in
the breathing loop fell below the 0.7 bar setpoint. This point should be
reached somewhere about -75m, which is at odds with the rescuer's report
that the solenoid opened during the ascent from -105m to -77m. It seems
probable that whatever was causing the solenoid to open was also causing
the rebreather's alarm to sound. Although this might seem to be a
peripheral issue, it establishes that the oxygen loss occurred during
the rescue, rather than earlier, and touches on the secondary question
of whether Włodek's had used his bailout switch before losing
consciousness.
The oxygen valve was not turned off by rescuers until the next day and it is unclear why the solenoid would have fired repeatedly, eventually emptying the oxygen cylinder of its contents, only after the rescuers came on the scene. One clue is provided on the French forum where Frédéric Badier reported [at 2005-04-08 20:07:41] that the oxygen cell compartment was flooded. Flooding of the cell compartment would explain why the cells no longer detected freshly injected oxygen and, therefore, would explain the repeated injections of oxygen.
This leads to the natural follow-on question: what caused the oxygen cell compartment to flood? Recall that Włodek would have been dead for over 24 hours before the first rescuer arrived on the scene, yet there was reportedly still oxygen pressure and there was no suggestion of the solenoid opening and the alarm sounding until the body was being moved up the shaft. I identify two main possibilities:
- The bailout valve was in the open-circuit
position when first found, indicating that Włodek had started a
possible bailout. In the open-circuit position the bailout valve
should not have allowed the breathing loop to become flooded, even
with the mouthpiece out of Włodek's mouth. However, Frédéric Badier
indicated that the rescuers lifted Włodek up the shaft "after
closing the mouthpiece". From what I can gather [the original
manufacturer has disappeared from the diving scene], it is not
possible to "close" such a bailout valve. It has only two positions:
open-circuit and closed-circuit. If by "closing the mouthpiece"
Badier means that the rescuers switched the bailout valve to its
alternative position, they could have inadvertently flooded the
rebreather, had it been in the open-circuit position when first
found. A problem with this scenario is that the official report
states that the bailout valve was provided to the expert witness in
the open-circuit position.
- The bailout valve was in the closed-circuit position when first found. Once the mouthpiece had left Włodek's mouth the breathing loop would have been open to the possibility of flooding. The fact that the three oxygen cells still showed ppO2 setting of around 0.9 bar when Włodek was found indicates that the oxygen cell compartment was not flooded at that point. Flooding could subsequently have occurred when the rescuers changed Włodek's attitude in the water, thereby causing the expulsion of air pockets. If the rescuers had, however, "closed" the bailout valve – in other words, closed off the breathing loop – before attempting to move the body, this scenario is less likely.]
In my opinion, the evidence tends to suggest that the rescuers found the bailout valve in the open-circuit position and, possibly not being familiar with the unit, moved ("closed") it to the closed-circuit position before moving the body. It would also make perfect sense to return the bailout valve to its original position before any forensic examination took place. As the official report concluded, the amount of diluent remaining suggests that Włodek used a portion of it in bailout (open-circuit) mode.
In spite of what I believe to be some shortcomings over interpretation of data, the French report nevertheless provides us with a wealth of factual information and (correctly, in my view) identifies the root cause of the accident: as being the wrongly formulated diluent gas. That said, I also believe that the report misdiagnoses the mechanism through which the bad diluent led to Włodek's death.
The two main questions therefore arising are:
- How did the bad diluent lead to a fatal outcome? and
- How did Włodek get to dive on such a clearly incorrect diluent?
The French report's author tries to form a plausible hypothesis to answer the first question, viz:
… during the descent the diver had to breathe 15/50 trimix from the beginning of the dive and to finish, in the deep exploration, on 10/70 trimix. Indeed, this mixture, being richest in helium (70%), is only 20% nitrogen, and should eliminate the problems of narcosis. Yet if he follows this procedure when, at a depth of around 80m to 90m, he injects air instead of a 15/50 trimix mixture, the narcotic effect of the nitrogen (nitrogen narcosis) is immediate...
The wording of this paragraph leaves unclear what the author is proposing, even allowing for the vagaries of translation. The most straightforward (and least likely) interpretation is that Włodek used the external 15/50 trimix directly through a demand regulator down to a depth of -80 or -90 metres [15/50 trimix exceeds a ppO2 of 1.3 at -86 metres], at which point he switched mouthpieces in order to breath from the rebreather. A second (more plausible) interpretation is that Włodek is supposed to have attached the 15/50 trimix cylinder to an inflation point on his rebreather's counterlung and used the gas as a diluent. At a depth of around -80m to -90m, he stopped using the external cylinder and started using the rebreather's internal diluent. He then injected what he thought was a 10/70 trimix and the narcotic effect of the new diluent was "immediate".
The relevance of this immediate narcotic hit is unclear because the author then suggests that Włodek, by then deeper down, responded appropriately to an alarm on the Inspiration as a result of the ppO2 exceeding 1.6 bar, in spite of apparently having already been overcome by narcosis higher up in the cave:
As the diver continues to descend on air, the ppO2 does not stop increasing [continues to increase?] proportionally with the ambient pressure, and the ppO2 of injection of the mixture exceeds the critical value of oxygen (1.6 bar) acceptable to the rebreather and the alarms trigger (audible and visual).
Mr. Szymanowsky, thanks to these alarms, sees the problem but analyses it as a malfunction of the solenoid valve, leading to hyperoxia. In that case, the recommended procedure is the following: etc, etc
Thus, it's not entirely clear what the author is trying to suggest. The relevance and modus operandi of the alleged narcotic hit somewhere between -80m and -90m are unclear and seem to be unconnected to the eventual cause of the accident.
Unfortunately, the hypothesis also does not fit the evidence particularly well and, as far as I can see, the rationale for the swift narcosis hit is not based on any hard evidence other than the author knowing that Włodek carried two external cylinders, one containing 15/50 trimix.
- As already mentioned, Frédéric Badier's
first-hand report states that both external cylinders were fully
operational but appeared to be untouched. If it is true that they
were untouched – and their rapid return to Poland, without further
analysis, lends weight to this interpretation – the hypothesis
cannot be correct. Włodek's diving colleagues have also confirmed
that the external cylinders were only there for bailout purposes and
not connected to the rebreather. And the brief report into the
accident at the plongeesout.com
site states:
Son diluant trimix, une bouteille externe au recycleur, n'est pas connecté, il plongeait à l'air.
[His trimix diluent, a bottle external to the rebreather, is not connected, he dived on air. [My emphasis.]]
Furthermore, on Włodek's "Deep and High" web site, in the page describing his trip to "Elefante Bianco" in Italy http://www.deepnhigh.pl/Włodek/Deep_+_High-_News/content_065.html he says:
"Na wypadek awarii rebreathera miałem ze sobą dwie awaryjne dziesięciolitrowe butle z nitroksem (Nx40) i trymiksem (Tx15/50)..."
[In the event of a rebreather failure, I had two 10-litre emergency bottles with nitrox (Nx40) and trimix (Tx15/50)... [My emphasis.]] - Even if we were to accept that the 15/50 trimix was being used as a diluent, at the postulated switch-over of diluents Włodek could have either continued to add incremental squirts of the new (bad) diluent to the breathing circuit as he descended or he could have flushed out the old 15/50 trimix with the rebreather's internal diluent. The author does not suggest which he believes occurred, but the incremental method is very unlikely to have given the suggested "immediate" narcotic effect, whereas the diluent flush is both wasteful of diluent and very likely to have immediately triggered a ppO2 alarm on the rebreather, given the diluent's composition.
Thus, if, as the evidence suggests, Włodek did not use the external cylinders and they were reserved for bailout purposes, the French expert's hypothesis regarding the rapid narcotic hit cannot be correct.
A further part of the author's hypothesis is that further injection of the diluent caused a ppO2 alarm deeper down which, in turn, caused Włodek to perform a diluent flush. For reasons that I will discuss in the next section, I also believe that this is incorrect.
10. An Alternative Analysis
As much as I would like to, it is not possible to give a definitive account of what happened, since much evidence is unavailable or has gone missing, and what evidence we have is either incomplete or inconclusive (or both). Nevertheless, I believe the following analysis provides a fairer idea of plausible scenarios, although much can only remain an educated guess.
In line with the Badier report and the view of his Polish diving colleagues, I believe that Włodek dived using only his rebreather and kept the two external cylinders only for bailout purposes.
We know that, when tested, the diluent contained 21.3% oxygen, 4.8% helium, with the remainder presumably nitrogen. In effect, it had a composition very similar to an air diluent.
One of the first questions regarding Włodek's dive is: which setpoint was he using in the deeper sections of the cave? The most conventional approach with the Inspiration rebreather is, as previously described, to use the low setpoint (usually 0.7 bar) for the first 20-30 metres and then move to the high setpoint for the rest of the dive. There are two pieces of evidence that suggest Włodek was using the low setpoint deeper down: firstly the official report states that he used a 0.75 bar ppO2 setting on his VR3 dive computer, and, secondly, in the French forum Xavier Méniscus [at 2005-04-11 18:49:16] states:
The ppO2 values on the slave computer were:
0.92 / 0.93 / 0.95
The slave computer was set to a setpoint of
0.70
the VR3 was set to 0.70
I could not turn the body to read
the right-hand instruments, master computer and O2 pressure
When
I brought him back from -105m to -77m, the buddy alarms started, and
[it] injected O2
In this type of accident, as Fred said, we
should be able to analyse the gas in the rebreather at the bottom before
recovering the body, for this [we need] to have a sampling system that
would collect a little gas from the interior of the bag.
At
-105m, I tested the diluent inflator (blue) and O2 (green), this worked
and sent gas, which allows me to say that the O2 bottle still contained
gas, without being able read the pressure gauge, on the other hand,
diluent was 120 bar
In spite of the small discrepancy between the official report (VR3 = 0.75 bar) and Xavier Méniscus's first-hand report (VR3 = 0.7 bar), Xavier Méniscus also reported that the slave controller was showing a setpoint of 0.7 bar. Thus, we can be reasonably sure that Włodek was using a low setpoint – somewhere around 0.7 bar – all the way down the cave.
When Włodek's body was found at a depth of -105m, Xavier Méniscus reported that
The ppO2 values on the slave computer were: 0.92 / 0.93 / 0.95.
which, although clearly above a 0.7 bar setpoint, was significantly below the 1.3 bar high setpoint for the rebreather – and well below the 1.6 bar alarm point. The low ppO2 readings strongly suggest that oxygen toxicity was not a problem and that no ppO2 alarm would have occurred.
Recall that the French report simply states that Włodek performed a diluent flush as a result of a ppO2 alarm but the author provides little evidence to support the hypothesis. The available evidence indicates that the ppO2 was significantly below the alarm point. A diluent flush will use a considerable amount of diluent when at depth. [I asked the Inspiration's manufacturer how much, but they did not respond to my e-mails.] The biggest objection to the report's hypothesis is that had Włodek performed a diluent flush the values on the oxygen controller should have been somewhere around 2.4 bar, given the composition of the diluent. Even allowing for the passage of 24 hours before the rescue diver reached Włodek's body, it is difficult to conceive of a mechanism that, in the absence of breathing, could have reduced the ppO2 from 2.4 bar to 0.9 bar.
It is possible to estimate that Włodek would have used somewhere around 30-40 bar of pressure from his (3-litre) diluent cylinder during his journey to -105m. We know from the French report that the diluent pressure was found to be 132 bar, suggesting a deficit of around 60-70 bar below what would normally be expected had the cylinder been full at the start of the dive [itself a speculative assumption]. The author concluded that Włodek therefore breathed a part of the diluent on open circuit. However, doing so would have used at least 70 bar of diluent per minute at that depth and very possibly considerably more due to stress or a CO2 breakthrough. Thus, the observed diluent deficit can be adequately explained by Włodek breathing diluent on open circuit for only a short time, without there having been a diluent flush. The diluent deficit also lends weight to the hypothesis that when the rescuers first found Włodek's body, the bailout valve was originally set to open circuit and was then switched to closed circuit by a rescuer, thereby causing the rebreather to become flooded. Since the report states that the bailout valve was in the open-circuit position, someone must have switched it back to its original position later on.
The question is therefore what situation might have caused Włodek to switch the bailout valve to open circuit yet did not allow him to make the crucial move over to his external bailout cylinders? I suggest that the reason for the fatality are likely to be found in a combination of the following factors:
- extreme narcosis-related problems; plus
- high gas density; possibly leading to
- CO2-related problems.
The deeper he went, the worse the problem(s) would have become. At some point during the descent of the shaft, his mental and physical capabilities became overwhelmed by one or more of the above factors and he reached a point where he was no longer in control of the dive. I have chosen -105m for the following calculations, since that is the depth at which the body was found, although it is quite possible that he ran into serious difficulty higher up the shaft.
Narcosis. It is possible to make a reasonably good estimate of the percentage of gases that would have been in the breathing loop, given a depth of -105m and reported ppO2 of 0.93 bar:
Oxygen = 0.93 / 11.5 = 8.1%
The remaining gases, helium nitrogen and exhaled
carbon dioxide, would have taken up the remaining 91.9%. For this
estimate, I will assume that the helium and nitrogen, which are not
metabolised by the body, will maintain a relative ratio of 4.8 : 73.9,
these numbers being the percentages of hydrogen and nitrogen found in
the diluent cylinder. [The ratio might be affected by differing rates of
absorption into tissue of each gas under pressure but should be
sufficient for this estimate.] Therefore
Helium = 91.9 * 4.8 / (4.8
+ 73.9) = 5.6% and
Nitrogen = 91.9 * 73.9 / (4.8 + 73.9) = 86.3%.
Thus, the nitrogen and oxygen would have made up around 94% of the breathing mixture. The amount of CO2 should have remained under 0.5% unless CO2 breakthrough had occurred. Had his diluent been a true 10/70 trimix, helium and nitrogen would have been 80.4% and 11.5%, respectively, so the narcotic gases would have made up only 19.6% of the breathing mixture.
There is no escaping the fact that, with or without a breakthrough of CO2, Włodek's breathing mixture was extremely narcotic, being almost five times higher, as a percentage, than it should have been.
Gas Density/Carbon Dioxide. The known facts indicate that there was at least a strong possibility of Włodek encountering a CO2-related problem at depth. With a combined oxygen/nitrogen level in his breathing loop of around 94% he would undoubtedly have experienced progressively greater difficulty in breathing as he descended, due to the combined densities of the two gases. As already discussed, this could lead to CO2 breakthrough in the scrubber as well as increased levels of CO2 retained within the bloodstream. Since we have a reasonable idea of the gas mixture he was breathing, we can estimate its density at a depth of -105m:
Oxygen: 11.5 * 1.33 * 0.081 = 1.24 g
Nitrogen:
11.5 * 1.17 * 0.863 = 11.61 g
Helium: 11.5 * 0.17 * 0.056 = 0.11 g
Total = 12.96 grams per litre
The actual density will depend on the temperature of the gas mixture and the amount of water vapour it contained. Water vapour is likely to be quite high in a closed-circuit rebreather and will reduce the density by a small amount. By contrast, surface-pressure air at 20ºC has a density of about 1.2 grams per litre, so Włodek's breathing gas at -105m would have been around ten times more dense. Had his diluent been a true 10/70 trimix, the breathing gas density at -105m would have been around:
Oxygen: 11.5 * 1.33 * 0.081 = 1.24 g
Nitrogen:
11.5 * 1.17 * 0.204 = 2.74 g
Helium: 11.5 * 0.17 * 0.715 = 1.40 g
Total = 5.38 grams per litre
so his actual breathing mixture was 2.4 times more dense than it should have been. Put another way, the density of his breathing gas at -105m was the same as diving to around -250m on a true 10/70 trimix.
There is a relatively famous case of a South African cave diver, Dave Shaw, who died while diving with a rebreather to a depth of 264m. The victim was trying to recover the body of a previously deceased diver and got into difficulties. A case study that was written about the incident [ http://www.ingentaconnect.com/content/asma/asem/2007/00000078/00000002/art00001] concluded that the probable cause of death was respiratory failure and CO2 narcosis. While I do not wish to suggest that this case exactly mirrors that of Włodek's death, there does seem to be a significant degree of overlap. Firstly, the density of the gas that Dave Shaw breathed at the bottom was calculated to be 10.2 grams per litre [I calculate 9.6 g/l using the 20ºC gas densities quoted elsewhere in this article], which is significantly less than the density of almost 13 g/l that Włodek would have experienced at less than half Shaw's depth. It is the gas density, rather than depth per se, that appears to have been the most significant factor in Shaw's death, so Włodek's situation was potentially even worse, even though his depth was less.
Secondly, there were questions about the packing of Shaw's scrubber absorbent. In Włodek's case there is the possibility that his use of unapproved, larger, cylindrical granules in the CO2 scrubber could have significantly reduced the surface area of its absorbent, and, due to the larger void sizes, potentially allowed earlier CO2 breakthrough when at depth. This, in turn, could lead to raised levels of CO2 in the breathing loop. Again, studies indicate that it is the gas density, rather than simple depth, that appears to be a critical factor affecting the efficiency of a rebreather's scrubber unit, so the risk of CO2 breakthrough would have been high in Włodek's situation.
It has been suggested that Włodek had used the same type of absorbent granules previously while diving in Elefante Bianco in December 2004 (dived to -100m) and Izbucul Tauz in January 2005 (dived to -85m). While this may well be correct, and the absorbent might have performed adequately during previous dives, it is nevertheless true that the use of a larger granule size with a different shape was very likely to have reduced the scrubber's efficiency, particularly at depth, and, with it, the rebreather's margin of safety. With an already reduced safety margin, the diluent used in the Goul du Pont dive had the potential to tip the balance in several ways. Firstly, the deeper he went, the progressively higher density of the breathing mixture would have significantly increased the WOB and therefore likely increased Włodek's production of CO2. Secondly, his MVV would have progressively degraded with depth and at -100m would have been only around one third that at the surface, significantly reducing his ability to expel any extra CO2 he was generating. And finally, the abnormally high density of the breathing mixture at depth is very likely to have significantly reduced the ability of the (probably) less efficient scrubber to absorb CO2 passing through it. Thus, there was the potential for CO2 build-up both in Włodek's bloodstream and in his breathing gas. The deeper he went, the greater the potential problem would become.
As well as often (but not always) causing a progressive increase in the rate of breathing, a high CO2 level can also have a narcotic effect on the diver, may increase susceptibility to (nitrogen/oxygen) narcosis and has been shown to increase sensitivity to oxygen toxicity. Anecdotal evidence also suggests that a CO2 breakthrough can occur very rapidly and with little prior warning, particularly when at depth. As Xavier Méniscus noted, it would have been useful to have taken a sample of the breathing mixture but they were not equipped to do so. It appears that the police also chose not to take a sample of the breathing mixture once the rebreather was on the surface.
There is an ongoing debate in rebreather circles as to whether a bailout valve should be connected back to the rebreather's onboard diluent cylinder or to an external cylinder. As was mentioned earlier, many rebreather divers argue that if the rebreather has malfunctioned, the diver should get off the system immediately and cannot rely on it any further to get out of trouble. In this case, Włodek had chosen to attach his bailout valve to the onboard cylinder. Given the circumstances of the accident, this was unfortunately a poor configuration.
The problem for Włodek was that the switch from closed to open circuit, using the internal diluent cylinder, would not have significantly changed the narcotic properties and gas density of the breathing mixture. Far worse, however, was that the ppO2 of the neat diluent he was now breathing would have immediately jumped from around 0.93 bar to 2.45 bar, taking him well into the oxygen toxicity danger zone. If he was already suffering from elevated CO2 levels, his sensitivity to oxygen toxicity is also likely to have increased.
By the time he came to a halt, presumably on a small ledge, at a depth of -105m, Włodek is likely to have been, at best, semi conscious and no longer able to operate his equipment. Although it appears he was still capable of turning the rebreather's bailout valve by a quarter turn, doing so would not have helped very much. The 60-70-bar diluent deficit suggests that he breathed on open circuit for less than 1 minute before losing the mouthpiece.
11. Diluent Mixture: A Disproportionate Blunder
To misquote a famous quotation, Włodek's death was worse than a tragedy; it was a blunder. This was no unexpected, out-of-the-blue occurrence that leads one to shrug one's shoulders and ponder on how "stuff sometimes happens". Rather, this was a completely avoidable death that resulted from a fundamental error being made, with, it has to be said, probably some help from Włodek himself.
The reason why Włodek dived on the bad diluent mixture remains a mystery to this day. One of the fundamental rules of diving is that you should always know what you're breathing, yet, for some reason, Włodek let his guard down and used a cylinder (or perhaps cylinders) containing diluent clearly not suited to deep diving.
The source of the bad diluent is not known. Włodek had dived at Izbucul Tauz back in January (to -85m), so we cannot discount the possibility that he simply chose to use his spare cylinder from the Tauz dive 2½ months later in the Goul du Pont. Sometimes it is also possible for the helium to leak out considerably faster than the other gases, even over a period of just a few months, but the proportions of gases found in the bad cylinder suggest otherwise and the resultant pressure drop would have alerted Włodek to the problem. This points to a bad fill, rather than helium leakage, being the source of the problem.
Thus, either the cylinder had been filled some time prior to Tauz or just before the trip to France. Either way, Włodek should have known the source of the gas mixture and it seems very probable that someone else also knew but, perhaps unsurprisingly, nobody has ever come forward with an explanation.
There seem to have been three main candidates for the bad diluent fill:
- The professional filling service in Warsaw that Włodek regularly used for his trimix fills.
- Włodek or a friend topped up/refilled the diluent cylinder, via a compressor, with the contents of a second cylinder that contained air, instead of a suitable trimix.
- Włodek or a friend attempted to blend the erroneous mixture from scratch.
Note that for options 2 and 3, we cannot exclude the possibility that Włodek did the fill himself.
11.1. Professional Service. In spite of all the gadgets he bought, Włodek had never acquired a diving gas analyser, not even one for oxygen. It therefore made good sense to use a professional filling service, which is what he normally did. For example, we know that he used a company in Warsaw to do a diluent fill of 10/70 trimix on 12/01/2005 for his trip to Izbucul Tauz, in Romania, and a bailout fill of 15/50 trimix on 13/12/2004 for his trip to Elefante Bianco, in Italy. It is worth noting that by this time he was no longer working in Warsaw, having left Siemens Financial, and was by then back in his home town of Wrocław, and without a job. Using the Warsaw-based filling service therefore required a time-consuming and quite expensive 700km round trip for Włodek or one of his colleagues.
We also know that Włodek took two diluent cylinders to France and that the one that was not used on the Goul du Pont dive (still) carries the label dated 12/01/2005, the date just prior to his Izbucul Tauz trip. What we do not know, because the French report inexplicably failed to record it, is the information on the red label of the diluent cylinder that Włodek used on his fateful dive, other than it was supposed to be a 10/70 trimix and had some white tape. The purpose of the white tape on the red label is unclear and there is no photograph to help clarify matters. These are critical omissions that make it difficult to identify the source of the fill.
From talking to local divers, the Warsaw filling service that he normally used seems to have been professional in its approach and people collecting freshly-filled cylinders were strongly encouraged to check the contents themselves before leaving. Thus, if he had used this service before going to France, he should have been able to check the mixture before he left the shop.
11.2. Top Up/Refill. Although he did not own a compressor, Włodek would very likely have had access to one. Recall that the report states that the diluent mixture contained 21.3% oxygen and 4.8% helium. At first glance, it suggests that the mixture was created by erroneously adding air to a cylinder that contained the remains of some kind of trimix. However, on closer inspection, the figures are a little odd because 21.3% oxygen is higher than that found in air (20.9%). Adding air, which contains 20.9% oxygen, to a trimix, which should always contain less than 20.9% oxygen, could never have created a mixture containing 21.3% oxygen. In fact, because there was still 4.8% helium in the mixture, the figure should be less than 20.9% if the refill gas was normal air. Although the author does not specify the make/model of the gas analyser, the report shows an Analox ATA Trimix Analyser in a number of photographs. The specification of this unit states that its O2 accuracy is "± 1% of reading and ± 0.2% of O2". [My interpretation of this is that the true oxygen level would have been somewhere between 21.1% and 21.5%.] This suggests that the unit's tolerance range cannot fully account for the discrepancy, although Analox have told me that it could simply have been a result of improper calibration by the user.
All things said, the figures are broadly in line with an almost empty trimix cylinder having been filled with normal air.
11.3. Gas Blending. The remaining possibility is that the gas mixture was created using a more complex blending technique. We know that Włodek neither owned a compressor, nor did he have the equipment needed to mix his own breathing gases. We do, however, know that the person who organised the April 2005 trip to France had a basic capability to mix breathing gases (and top-up/refill cylinders), including trimix, although we do not know whether Włodek used his equipment or expertise.
Thus, there were three possible ways in which Włodek might have filled his diluent bottle(s) – and very little evidence as to which one he used. We do know that the diluent cylinder used on the day of the accident carried a red label stating that it contained a 10/70 trimix, but that does not preclude the possibility that it had been refilled at a later date, either by Włodek or by a friend, and the presence of white tape on the red label is an additional mystery. [Knowing the fill-date on the label might have helped in this respect because Włodek had apparently not dived since January 2005.]
The only thing to add is that the person who held on to Włodek's cylinders, including the second diluent cylinder, waited for some time before eventually returning them to Włodek's widow. By that time, along with the two spare 3-litre cylinders for the Inspiration, he had also taken possession of the two 10-litre bailout cylinders that had been repatriated along with Włodek's body. However, before returning the four cylinders, he did something that is puzzling:
- he emptied the 3-litre diluent cylinder of its contents; and
- he then removed the pillar valve from the cylinder and replaced it with a threaded plastic stopper.
While the reason for these actions remains unclear, the presence of the plastic stopper made it clear that the cylinder had been open to the atmosphere for an indeterminate length of time. Given the potential importance of this cylinder in helping to identify the source of the bad diluent mixture, it was a questionable action. The other three cylinders in the person's custody were returned untouched.
Thus, the source of the bad diluent mixture must remain a matter of speculation. The French report omitted critical information and the contents of the second diluent cylinder were emptied for reasons that have never been explained. As for re-examining the cylinder used on the fateful dive, that too is no longer possible...
Once the French report was published, attempts were made to find out who might have filled the diluent cylinder. Investigations came rather unstuck, however, when it was revealed that both of the rebreather's cylinders, which were still being held in the custody of the French authorities, had *cough* "gone missing". It was then found that the spare diluent cylinder, by then back in Poland, had been emptied of its contents. When arrangements were subsequently made for someone to collect the rest of the Inspiration rebreather and transport it back to Poland, the reader will no doubt be deeply shocked to hear that it too had "gone missing" from French custody, never to resurface. And the two dive computers remaining in French custody? Also libérés, it seems.
12. Conclusions
So far, I have tried to shed some light on how an inappropriate diluent and unapproved CO2 absorbent could have led to a fatal outcome. What I have not yet covered is why Wlodek came to use an air diluent in a deep cave. Once again, I do not claim to have the answer. Nevertheless, we can glean some possibilities from the available facts.
Some time ago, I came across a scrap of paper amongst Wlodek's personal effects on which someone had written:
Ardeche -
Goul de la
Tannerie
Goul du Pont
Aside from its poignancy, it seemed to tell me nothing I didn't already know. Quite some time elapsed before I eventually understood the message it conveyed: that the trip to France was organised with two caves in mind. By focusing on the Goul du Pont, where Wlodek had died, I had neglected the previous day's dive in the Goul de la Tannerie.
The Goul du Pont and the Goul de la Tannerie are both deep, flooded systems but have rather different depth profiles. Whereas the former quickly gains depth, the latter contains a horizontal, flooded gallery with a depth varying between -3m and -10m for its first 700m, before it then rapidly heads off down to an explored depth of over -220m.
Recalling our Rebreather 101 lessons, a diluent should be able to sustain life when breathed directly so as to allow for the possibility of diluent flushes and bailout using the onboard diluent cylinder. Thus, for shallow dives a 10/70 trimix is unsuitable and an air diluent is to be preferred (and considerably cheaper), with the more expensive trimix diluent mixtures reserved for deeper dives. As well as being unnecessarily expensive, a 10/70 trimix will be hypoxic if breathed directly at depths above -6m, making it potentially unsafe for use during the first 700m of the Goul de la Tannerie.
We know that Wlodek's maximum recorded depth on his dive in the Goul de la Tannerie was only to -9.4m, so it is clear that he never ventured beyond the horizontal gallery. While we don't know how deep he had planned to go in the cave, this suggests that he should have chosen an air diluent in the gallery both for reasons of safety and cost.
Thus, when preparing for his trip to Bourg Saint Andéol it is reasonable to expect Wlodek to have taken two diluent cylinders – which we know he did – with one containing air for the Goul de la Tannerie and the other a trimix for the Goul du Pont. Whether he had two different mixtures is unknown, but there can have been only two possible permutations: one air plus one trimix or both air. [We know from the French report that one cylinder contained air but the second cylinder's mixture is unknown, having been inappropriately emptied by a Polish diver.] Represented symbolically, the permutations are T1 + A2 or A1 + A2, where A is air, T is trimix and the 1/2 is the cylinder number. The cylinder used on the fatal dive is A2.
From these two possible permutations, we can derive three possible usage scenarios: A1 + A2, T1 + A2 and A2 + A2.
A1 in Goul de la Tannerie and A2 in Goul du Pont. Had both cylinders contained air, this would almost certainly indicate a monumental screw-up during the filling stage.
T1 in Goul de la Tannerie and A2 in Goul du Pont. This is the classic mix-up. Unless he had needed to perform a diluent flush or breath directly from the onboard diluent, Wlodek would have been able to use the 10/70 trimix in the Goul de la Tannerie without incident. He then swapped diluent cylinders the next morning, prior to his dive in the Goul du Pont.
A2 in Goul de la Tannerie and A2 in Goul du Pont. In this scenario Wlodek used the air diluent in the Goul de la Tannerie but did not change cylinders prior to diving the next day. For this to have occurred, Wlodek would have either believed that the first day's dive was on trimix [and therefore believed he had two trimix cylinders] or he simply forgot to change cylinders the next morning.
There is the unexplained mystery of the white tape on the rebreather's diluent bottle. Since we know that both cylinders still sported red 10/70 trimix labels, it follows that unless Wlodek believed he had two trimix cylinders, there would/should have been some kind of marking to identify which was air and which was trimix. Whether the white tape was such an identifier is just speculation but, if the two cylinders held different diluent mixtures, some system would have been necessary to indicate which was which. This raises the intriguing and equally disturbing possibility that the cylinders might have been mislabelled or details of the labelling system used were simply miscommunicated.
When doing research for this article I came across some salutary words of warning that stayed with me. They are attributed to a gentleman named Richard Bull, who said: "most rebreather accidents have already occurred before the diver gets in the water – it’s just that the diver hasn’t realised it yet.". It's hard to argue with the Mr Bull's logic in the case of Włodek's death.
Unfortunately, there were identifiable vulnerabilities in Włodek's diving set-up:
-
In spite of all the diving-related gadgets that he had bought, he never owned a gas analyser. While helium and trimix analysers are (and were) relatively expensive, oxygen analysers are (and were) considerably cheaper. Given the importance of knowing how much oxygen is in a breathing mixture, this critical omission is difficult to understand. As already discussed, it is ultimately the diver's responsibility to know what gas he will be breathing, yet Wlodek seems to have skipped this vital test. Instead, there is the disturbing possibility that he was relying solely on a simple indicator, possibly just a piece of white tape, to identify the mixture in each cylinder.
-
He was using an unapproved granule size of CO2 absorbent, which he apparently had used before. This apparently inconsequential increase in granule size could have reduced the effective surface area of the absorbent by up to half, and significantly increased the potential for CO2 breakthrough at depth. Although it has been suggested that he thought it performed better and had successfully used the same absorbent on earlier dives, he was nevertheless taking a calculated risk using it.
-
His bailout valve was connected back to the rebreather's internal cylinder. While many other rebreather users have the same set-up, it probably had fatal consequences for Włodek in this instance.
Given the situation he found himself in, he should have turned back before his situation became overwhelmingly critical, although we cannot ignore the strong possibility that his analytical faculties were already affected by narcosis. That said, once he was engulfed by the crisis, I believe the only way he could have survived is if he had earlier chosen to connect the bailout valve to an external cylinder. While a bailout mixture suited to the maximum depth he intended to reach – probably a 10/70 trimix – would have been preferable, his existing 15/50 trimix would have been acceptable. Of course, such a line of reasoning only makes sense once we know that the onboard diluent bottle did not contain a 10/70 trimix...
When I hastily wrote the obituary for Włodek back in April 2005 [ http://www.oucc.org.uk/dtt/vol15/dtt15_07.htm] I identified his fondness both of risk taking and of gadgets as factors that would have drawn him to cave diving. Almost ten years later I still think it was a valid observation. However, I now also believe that his natural propensity to take risks had not become sufficiently tamed by the discipline required of the cave diver. While many of us will have abseiled on well-frayed harnesses or used karabiners that have clearly seen better times, we know that there is still a fair margin of safety in the system. Cave diving reduces the safety margin by a considerable degree and cave diving on a rebreather arguably even more so. In short, it is a potentially unforgiving environment where being a tad obsessive-compulsive can be a positive benefit, and taking chances and thinking that you can “wing it” can be incompatible with survival. Unfortunately, I believe Włodek never really shook off his old ways during the move to cave diving. Those who knew him would probably agree that his personality was very far removed from being obsessive-compulsive. Sadly, that might very well have contributed to his eventual undoing.
Appendix A: Original Text of French Report Summary
Les éléments recueillis au cours de notre expertise ne mettent pas en évidence de dysfonctionnement du recycleur pouvant un accident de plongée
En revanche l'erreur de mélange dans la composition du recycleur est l'origine de l'accident.
Cette erreur est d'autant plus fatale qu'au cours de la descente le plongeur devait respirer dès le début de la plongée le Trimix 15/50 pour finir, au plus profond de son exploration, sur le Trimix 10/70. En effet, ce mélange, étant le plus riche en Helium (70%), n'a que 20% d'Azote, ce qui anhile les problems de narcose. Or s'il respecte cette procedure quand il injecte au alentour des 80 a 90 m de l'air, au lieu d'un mélange Tx 15/50, l'effet narcotique de l'Azote (ivresse des profondeur) est immédiat. Les plongeurs au recycleur sont plus sensibles a la narcose car la Pp O2 étant inferieure par réglage a celle obtenue en circuit ouvert entraîne une Pp N2 nettement supérieure.
Aussi pour ces raisons, le constructeur du recycleur limite la plongée a l'air a 50m; non seulement pour l'intoxication a l'Azote (N2) mais aussi pour celle a l'oxygène qui pourrait en découler. De plus comme le recycleur Buddy fonctionne avec des valeurs d'oxygène comprise entre 0,75 b (Set point bas) et 1,6 bar (Set point haut), au dela de 50m la gestion électronique du recycleur ne peut ,maintenir la PpO2 dans cette fourchette en raison de l'augmentation de la pression ambiante.
De ce fait, au-delà de 50m le plongeur doit utiliser un mélange Trimix ou Heliox.
De plus, ceci s'associe a une augmentation très rapide de la PpO2 dans la boucle qui devient en application de la loi de Dalton, très supérieure au 1,6 bar autoriser par la machine.
Comme le plongeur continu de descendre avec l'air, la PpO2 ne cesse d'augmenter proportionnellement à la pression ambiante et la Pp O2 d'injection du mélange dépasse la valeur critique d'oxygène (1,6 b) admissible dans le recycleur et les alarmes s'enclenchent (sonore et visuelle).
M. SZYMANOWSKY, grâce a ces alarmes, constate
le problème mais il analyse comme un dysfonctionnement de son
electrovanne et entraîner une hyperoxie. Dans ce cas, la procédure
préconisée est la suivante:
– Regarder l'affichage pour
juger si la PpO2 grimpe rapidement ou si elle résulte d'un pic cause par
une descente trop rapide.
– Si elle continue de grimper,
fermer la bouteille d'oxygène et faire diminuer la PpO2 en rincant la
boucle a l'aide de l'inflateur de diluant.
– A l'issue de ce
rincage, inspirez et re ouvrez la bouteille d'O2 tout en surveillent la
PpO2. Si elle grimpe,a nouveau, le solenoide est bloque en position
ouverte alors refermer la bouteille d'oxygène.
– Pour
continuer d'utiliser le recycleur, il faut ouvrir et fermer le robinet
d'oxygène sur de courts instants tout en contrôlant l'apport d'O2. Meme
si cela n'est pas très pratique, le recycleur peur être utilise aussi
longtemps que necessaire mais la solution est d'utiliser les bouteilles
de secours en circuit ouvert (bail out).
M. SZYMANOWSKY applique cette procedure. Cette manoeuvre reste inefficace car la Pp O2 d'injection du diluant est supérieure a celle admissible par la machine. Aussi, la victime ne peut que de basculer, la vanne quart de tour, de son embout Eisberg K 96 en circuit ouvert. C'est ce qu'il fait (embout en position bail out valve) mais la bouteille d'alimentation n'est pas adaptee a la profondeur d'évolution car elle est très narcotique et hyperoxique.
Meme s'il est de coutume en plongée souterraine de plonger seul, M. SZYMANOWSKY aurait pu éviter cet accident s'il etait accompagne d'un plongeur en scaphandre autonome en lui fournissant un mélange gazeux en adequation avec le profondeur.
Appendix B: Selected Quotations from "Plongée Souterraine" Forum
2005-04-08 20:07:41 (Fredbadier)
Le Secours de Bourg St Andeol géré par le SSF s'est terminé cette
après midi dans de bonne conditions. Le corps de Wlodec a été remonté à
la surface par l'équipe mise en place par le SSF.
Le corps a
été retrouvé à -105m. Les causes de l'accident ne sont pas établies. Le
procureur décidera des suites de l'enquète.
Quelques faits sur la base des observations faites en immersion par les plongeurs du SSF puis en surface lors de l'inspection réalisées par les plongeurs habilités de la gendarmerie. Je précise que les plongeurs spéleo impliqués ne sont pas des experts buddy ni de formation Buddy. Il se peut que le texte qui suit comporte des erreurs. Merci de le prendre en compte. Il ne s'agit pas d'un compte rendu des plongées du SSF. Le SSF produira sans doute un rapport.
Lors de la découverte du corps, le plongeur
n'avait plus son embout de recycleur en bouche. L'embout équipé d'un
2ème étage était en position recycleur. La bouteille de diluant était à
120 bar lors du retour en surface. Le VR3 indiquait un trimix 10/70 et
était en mode circuit fermé avec PpO2 (setpoint) à 0.70 bar. Lors de la
découverte du corps, l'écran du buddy esclave était opérationnel et
indiquait des valeurs de 0.90 à 0.92 pour les cellules. L'écran du
maître n'a pas été inspectée. Lors de la remontée du corps à -80m,
l'alarme du buddy a bippé et l'injection d'O2 s'est enclenchée. Le corps
a été déposé à -80m dans l'attente de la plongée de récupération qui à
eu lieu le lendemain. L'électronique du buddy (maître et esclave ) ont
été laissé en l'état ( en marche); Seul les relais ont été remonté à ce
stade
Il est probable ( il s'agit d'une hypothèse) que le
recycleur a tenté toute la nuit de réguler le taux d'oxygène. Après la
plongée de récupération, le plongeur a été inspecté en surface. Les
ordinateurs du buddy étaent éteints et n'ont pu être remis sous tension
et la bouteille d'o2 était vide.
Nous supposons ( hypothèse
encore une fois) que la batterie du buddy a été vidée lors des
tentatives constante de régulation de la PpO2 dans la nuit. Il n'a pas
été possible de connaître le setpoint PpO2(consigne) choisi du
recycleur.
Le recycleur était noyé y compris le
compartiment des cellules ce qui peut s'expliquer par le lacher d'embout
et l'immersion longue du recycleur dans de telles conditions
(interprétation)
Les inflateurs O2 et diluant étaient
opérationnels. La bouteille de diluant ne comportait pas de marquage
quand à la nature du gaz. Aucune analyse n'a était faite sur le site,
les gendarmes prenant en charge cette opération.
les lampes du plongeur étaient
opérationnelles ainsi que le 2ème étage intégré dans l'embout. L'air II
sur la bouée était opérationnel. le recycleur était équipé d'un
répétiteur à 3 leds sur l'embout (dans le visuel du masque). Le
recycleur comportait un kit pour une 4ème cellule avec cable de
connection pour le VR3. Ce câble n'était pas utilisé. Nous ne savons pas
si une cellule était en place (peu vraisemblable sinon il aurait été
connecté:: hypothèse encore).
En plus du recyleur , le
plongeur avait 2 relais qui n'ont pas été utilisés (embout lovés sur la
bouteille). Un bloc d'environ 2L était fixée sur le haut de l'appareil
derrière la tête du plongeur. Il servait pour le gonflage du vêtement.
Ce système était opérationnel. La chaux avait été changée avant la
plongée, le reste du bidon a été saisi par la gendarmerie pour analyse.
Difficile de conclure sur les causes de
l'accident, rien ne nous a paru anormal. On peut émettre 3 hypothèses
(ce ne sont que des hypothèses):
-Malaise du plongeur?
-Dysfonctionnement de l'appareil et erreur dans l'affichage de la
teneur en O2 du buddy ?
-Mauvaise calibration en surface
conduisant a une impossibilité de réguler la PpO2 pour le buddy
Nous ne connaissons pas la vitesse de descente du plongeur ( analyse du VR3 à faire) qui aurait pu faire monté la PpO2 très vite.
Selon les équipiers de Wlodec, il plongeait avec le buddy depuis plus de 2 ans et avait plusieurs centaines de plongée avec le buddy dont certaines dans les mêmes tranches de profondeur. Il avait une expérience en buddy et a fait sa calibration avant la plongées;
Je conçois que ces détails soient un peu
froids et peu humain. Je m'en excuse. J'essais d'être le plus factuel
possible; Je compatis avec la famille de Wlodec ( il laisse 1 femme et 3
enfants) ainsi que ces proches. La nouvelle nous attriste et j'adresse
toute mes sympathies a ceux-ci. En espérant que nous puissions
comprendre les causes et prévenir des accidents similaires. Mais cette
leçon si elle est possible ne nous ramèneras le plongeur disparu et ne
vaut une telle perte.
Fred
2005-04-12 18:25:47 (Xavier Méniscus)
"Un autre piste peut-être le CO2 : chaux mal conditionnée, oubli de
remettre un joint ou l'entretoise,"
Le joint et l'entretoise étaient en place, lorsque nous avons démonté le buddy.
A+
Xavier
2005-04-12 18:33:53, (Fredbadier):
Le joint et l'entretoise était en place, nous avons vérifié. De plus
je pense qu'en cas de probleme CO2 le plongeur aurait basculer en ouvert
son embout le permettait.
Comment fait le Buddy pour
detecter des sondes fatiguées. Verifie t'il le voltage des cellules sur
10¨% d'O2 et si ces voltages sont hors normes alors la calibration
echoue?
Je ne voie pas en quoi un écart ds le viellissement
des cellules est un problème dans le remplacement de cellules non
simultané sauf si l'une d'elle est HS.
Je ne pense pas que l'expertise du materiel aille bien loin, les gendarmes d'Oloron St Marie avaient des doutes sur le fait que le procureur allait pousser l'enquète du fait qu'il ne s'agisse pas d'un ressortissant Français et des couts associés...
Je ne sais pas si les discussions sur ces points techniques sont à leur place sur le forum. Peut être vaut il miuex en discuter sur une liste recycleur?
Bonnes Plongées (avec des petites bulles...)
2005-04-11 18:49:16] (Xavier Méniscus):
Salut
Les valeurs de PpO2 sur l'ordinateur esclave
étaient de : 0,92 / 0,93 / 0,95
L'ordinateur esclave était réglé
pour un set point à 0,70
le VR3 était réglé à 0,70
Je n'ai pas pu
tourner le corps pour lire les instrument coté droit, ordinateur maitre
et pression O2
Lorsque je l'ai remonté, de -105m à -77m, les
alarmes du buddy se sont mise en route, et ont injecté de l'O2
Dans ce type d'accident, comme le dit Fréd, il faudrait pouvoir analyser
le gaz contenu dans le recycleur au fond, avant de remonter le corps,
pour cela avoir un système de prélèvement qui permettrait de prélever, à
l'interieure des sac, un peu de gaz.
A -105m, j'ai testé les
inflateurs de diluant ( bleu ) et d'O2 ( vert ), ceci fonctionnait et
envoyait du gaz, ce qui me permet de dire que la bouteille d'O2
contenait encore du gaz, sans avoir pu lire le mano, par contre, le
diluant était à 120 bar.
A+
Xavier